CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
TECHNICAL TIPS
Embolectomy
Use an operating table that allows x-ray penetration. Local anesthesia is used if embolus is likely and the obstruction seems to be in the upper thigh or in pelvic vessels (no pulse in the groin). Make a longitudinal incision in the skin, and identify and expose the common, superficial, and deep femoral arteries . If the common femoral artery is soft-walled and free from arteriosclerosis – especially if a pounding pulse is felt proximal to the origin of the deep femoral artery – an embolus located in its bifurcation is likely. Make a short transverse arteriotomy including almost half the circumference. Place the arteriotomy only a few mm proximal to the origin of the profunda artery so it can be inspected and cannulated with ease. In most other cases, a longitudinal arteriotomy is preferable because it allows elongation and can be used as the site for the inflow anastomosis of a bypass. For proximal embolectomy, a #5 catheter is used.
Before the catheter is used the balloon should be checked by insufflation of a suitable volume of saline. Check the position of the lever of the syringe when the balloon is starting to fill, which gives a good idea of what is happening inside the artery. Wet the connection piece for the syringe to get a tight connection. It is smart to get external markers of the relationship between the catheter length and important anatomical structures; for example, the aortic bifurcation (located at the umbilicus level), the trifurcation level (located approximately 10 cm below the knee joint), as well as the ankle level. The catheters have centimeter grading, which simplifies the orientation.
It is common for the embolus to already be protruding when the arteriotomy is done and a single pull with the catheter starting with the tip in the iliac artery is enough to ensure adequate inflow. This means that a strong pulse can be found above the arteriotomy, and a pulsatile heavy blood flow comes through the nole. For distal clot extraction, a #3 or #4 catheter is recommended. A slight bending of the catheter tip between the thumb and index finger might, in combination with rotation of the catheter, make it easier to pass down the different arterial branches (Fig. 8).
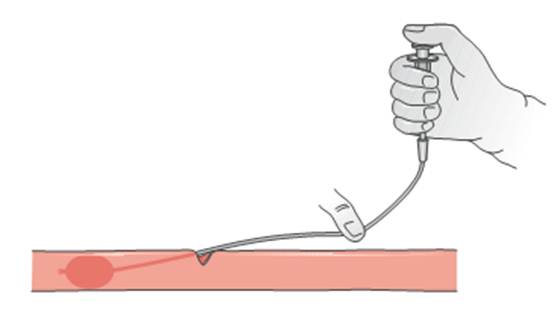
Fig. 8. Use of Fogarty catheter for embolectomy. Note that withdrawal is parallel to the artery
When the catheter is inserted into the artery and while the surgeon is working with it, hemostasis of the arteriotomy is achieved by a vessel-loop or by a thumb–index finger grip over the artery and the catheter. In a typical case, an embolus, including a possible secondary thrombus, can be passed relatively easily or with only slight resistance. If a major part of the catheter can be inserted the tip will be located in one of the calf arteries, most probably the posterior tibial artery or the peroneal artery. The balloon is insufflated simultaneously as the catheter is slowly withdrawn, which makes it easier to get a feeling for the dynamics and to not apply too much pressure against the vascular wall.
A feeling of “touch” is preferable, but a feeling of “pull” against the vascular wall should be avoided.
To get the right feeling the same person needs to hold the catheter, pull it, and insufflate the balloon at the same time. To avoid damage in the arteriotomy, the direction of withdrawal should be parallel with the artery .
When the catheter is withdrawn it moves into larger segments of the artery and has to be successively insufflated until it reaches the arteriotomy. The reverse is, of course, valid when the embolectomy is done in a proximal direction. The thromboembolic masses can be suctioned or pulled out with forceps, and the arteriotomy should be inspected to be clean from remaining materials before the catheter is reinserted. The maneuver should be repeated until the catheter has been passed at least once without any exchange of thromboembolic materials and until there is an acceptable backflow from the distal vascular bed.
Depending on the degree of ischemia and collaterals, the backflow is, however, not always brisk.
If a catheter runs into early and hard resistance, this might be due to previously occluded segment that forced the catheter into a branch. It should then be withdrawn and reinserted, using great caution to avoid perforation. If the resistance cannot be passed and if acute ischemia is present, angiography should always be considered to examine the possibility of a vascular reconstruction.
Besides performing embolectomy in the superficial femoral, popliteal, and calf arteries, the deep femoral artery must be checked for an obstructing embolus or clot that needs to be extracted. Separate declamping of the superficial femoral and deep femoral arteries to check the backflow is the best way to do this. Remember the possibility that backflow from the distal vascular bed after embolectomy might emanate from collaterals located proximal to distally located clots. Back flow does not always assure that the peripheral vascular bed is free from further embolic masses. A basic rule is that every operation should be completed with intraoperative angiography to ensure good outflow and to rule out remaining emboli and secondary thrombus. To dissolve small amounts of remaining thrombus local infusion of 2–4 cc recombinant tissue plasminogen activator (rtPA) can be administered before the angiography catheter is pulled out.
Finally, the arteriotomy is closed. If necessary a patch of vein or synthetic material is used to avoid narrowing of the lumen. As mentioned before, the embolectomy procedure includes intraoperative angiography. If this examination indicates significant amounts of emboli remaining in the embolectomized arteries or if the foot still appears as being inadequately perfused after the arteriotomy is closed, other measures need to be taken. If there are remaining emboli in the superficial femoral or popliteal arteries, another embolectomy attempt from the arteriotomy in the groin can be made. Clots, if seen in all the calf arteries, need to be removed through a second arteriotomy in the popliteal artery. This is done by a medial incision below the knee; note that localanesthesia is not sufficient for this. It is usually necessary to restore flow in two, or occasionally in only one, of the calf arteries.
Embolectomy at the popliteal level is the first treatment step when ischemia is limited to the distal calf and foot and when there is a palpable pulse in the groin or in the popliteal fossa.
Date: 2014-12-29; view: 1387
| <== previous page | | | next page ==> |
| Operation | | | Intraoperative angiography |