CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
The radio diagnostics of the musculosceletal system’s tumours
Section contents:
The radio signs of bones tumours are benign tumours (chondroma, osteoma, osteohondroma, solitar bone cyst, giant-cell tumour), primary and secondary malignant tumours (osteogenic sarcoma, Ewing`s sarcoma, osteoblastoclastoma, metastases).
The malignant and benign tumours of bones are distinguished.
Benign growth: regular shape of tumour, its correct structural picture, signs of slow growth, acutely outlined contours, clear marked off from a normal bone.
Signs of malignant growth: wrong form of tumour, destruction of bone tissue with formation of defect, blastomatosis needle or overlap periostitis.
The benign tumours of bones
Osteoma (see fig 13.1). Distinguish: spongy osteoma which consists of spongy substance and compact osteoma from the compactsubstance. Roentgenologically: correct structural picture, the cortical substance of tumour makes direct continuation of cortical substance of bone, violation of integrity of cortical layer in osteoma is not present, the spongeous structure of bone and tumours also without difficulty pass one to the other, contours of tumour are smooth and even, osteoporosis is always absent. The compact osteomas are mainly localized in flat bones, spongy and mixed ones - in tubular bones.
Osteochondroma except for a bone contains cartilaginous tissue too. The picture of osteochondroma is non-homogeneous, consists of correct bone itself, fan-shaped bunches and septums, that lie among the light background of the cartilage. Often original appearance reminds a "cauli-flower".
Hondroma (see fig 13.2). Depending on the direction of the growth distinguish enchondroma (in a bone medullar channel), and ekchondroma (bones grow on a bone surface). More frequent small cylinder bones are struck. On a sciagram every tumour consists of transparent cartilaginous background which characteristic itself are selected on, points from a lime or bone substance. Swelling is the leading syndrome of enchondrom, the external contours of hondroma are always clear, not interrupted while a tumour remains benign. A cortical layer is thinned, ekchondroma remooves extend the distance be ween the opposite departments of cortical substance. Hondromas are complicated by the pathological fractures and often become to malignant
Fig.13.1The compact osteoma

Fig.13.2 Chondroma of humeral bone
Gemangioma( see fig 13.3). More frequently is localized in a column; there are cavernous and capillary forms. In cavernous gemangioma the structure is changed due to the presence of vertically directed rough and thick trabecules, which remind columns. Capillary gemangiomas form a small-gause picture. The vertebral disks are not changed, pathological fractures are possible.
Giant cells tumour (see fig 13.4) built from the cells of two types - too characteristic giant multi-nuclear and shallow uninuclear ones. They are mostly in the age of 20-40 years, one localized in long tubular bones, in the bones of pelvis, lower jaw, and ect. At the small-gause form roentgenologically swelling and deformation of metaepiphysis end of the bone is determined.

Fig.13.4 The giant-cell tumour of tibia bone

Fig.13.3 Gemangioma
A structural picture forms the picture of small-gause or big-gause (cellular) brihgtness separated by thin boneseptums. The area of defect reaches to the joint surface and is separated from it by a dense subhondral plate. A cortical layer is outside and acutely thinned. The periostal reaction is absent. A regional unstructional defect with the expressly outlined contour appears in a lythical form. A cortical layer sometimes resolves fully, but from the side of connective tissues a defect can be limited by thin squamous shade - wall of the education. Malignisation often comes.
Tumour-like disease - the isolated bone cyst is more frequent localized in metaphysis of long tubular bones. Roentgenologically: in a metaphysis of tubular bone the limited area of the promoted permeability of rays of oval, fusiform with the expressly outlined contours is determined. On this area a bone is blown away, extended in width, the cortical layer is acutely thinned, but non interrupted. The reaction of periosteum is absent. Often on a background of the cyst linear shades of thin bone partitions, which divide it into the row of chambers of a different size, are revealed. A cyst is often complicated by the pathological fracture which heals well by a formation of dense periostal callosity with a next gradual filling of cavity of cyst normal bone by tissue.
Primary malignant tumours
Periostal sarcoma (see fig 13.5) develops from the external fibrous layer of periosteum. On a sciagram small intensive additional shade on the background of connective tissues appears. From the side of the bone a small superficial regional defect (ousura) with the thinned cortical layer, the contour of which remains even, is determined.

Fig.13.5 Periostal osteosarcoma sciagram and CT
Osteogenic sarcoma. It is extraordinarily malignant tumour. Osteolythic, osteoblastic and mixed types are distinguished.
In the osteolythic type( see fig 13.6) are osteoclastes malignanized, on a sciagram the area of destruction is determined in a metaepyphysis tubular bone as unstructural defect with unequal, jagged, like eaten contours. Often there is "overlap periostitis".

Fig.13.6 Osteolythical sarcoma the sciagram and MRI

Fig.13.7 Osteoblastic sarcom
In an osteoblastic type (see fig 13.7) there is blastomatosis as maculation shades of different form and size located in the area of a tumour, needle periostitis develops in the area of defect.
At the mixed type (see fig 13.8) of osteogenic sarcoma, various combination of destruction takes place and pathological /malignant/ bone-formation. In the place of tumour a bone fusiform is thickened, a cortical layer is blasted, is often observed needle or overlap periostitis.
Osteogenic sarcoma does not destroy cartilages, and in children and youths, the defect does not spread outside of epiphysar cartilage.
The paraostal sarcoma (see fig 13.9). The tumour develops from periost, consists of rough periostal stratifications of unhomogenous structure, a cortical layer is unchanged.

Fig.13.8 Mixed sarcoma

Fig.13.9 The paraostal sarcoma, hondromas in connective tissues of shoulder
Ewing’s tumour (see fig 13.10). It appears from reticuloendotelial tissue, more frequent in people under age of 20 years. Mainly long tubular bones are struck; quite often a tumour is localized in flat bones (iliac and other.). A clinical picture reminds acute osteomielitis - the disease begins with a high temperature acutely and is accompanied by leucocytosis. Gradually increasing pain appears, and locally edema in the area of which the skin of hyperemied and hot by a touch, appears. Roentgenologically in the defect of long tubular bones there is expansion of bone medullar channel; a cortical layer exfoliates as the longitudinal linear shades limited by light fissurel intervals. In future tender periostal stratifications, that surroud a bone like a shell, appear from the side of periosteum. These stratifications collapses, and periosteum again calcified, that creates the picture of the striped stratifications. Simultaneously there is the unclear outlined fusiform focus of destruction of bone tissue. Unlike osteomielitis, sequestrums, as a rule are absent. In the row of cases there are the original periostal changes in the type of thin and tender shades of needle periostitis. The damage of flat bones the changes have mostly a destructive character as an area of uneven destruction of spongy substance and differ a little from the picture of osteogenic sarcoma. The feature of Ewing`s tumour consists in high radiosensitivity, that is often used in difficult differential diagnostics. A tumour can give metastases into the other bones.
Myeloma (see fig 13.11) is the malignant tumour of marrow. The following varieties are distinguished: 1) plural-focuses; 2) diffuse-porotical; 3) osteosclerotical; 4) it is isolated (solitar). Myeloma destroys bone tissue.Roentgenologically: the plural rounded defects appear, by a diameter from some millimetres to some centimetres with sharp contours of every separate defect (punch defects). There are no reactive changes from the side of surrounding tissues.

Fig.13.10 Ewing’s sarcoma.
 Fig.13.11 Myeloma
Fig.13.11 Myeloma
 The secondary (metastatic) malignant tumours.(see fig 13.12) Most often metastases in bones give the tumours of prostate, lungs, gastrointestinal tract, uterus, thyroid gland and hypernephroma. Distinguish: osteolythical, osteoblastical and mixed metastases, which by the structure do not differ from osteogenic sarcomas.
The secondary (metastatic) malignant tumours.(see fig 13.12) Most often metastases in bones give the tumours of prostate, lungs, gastrointestinal tract, uterus, thyroid gland and hypernephroma. Distinguish: osteolythical, osteoblastical and mixed metastases, which by the structure do not differ from osteogenic sarcomas.
1  2
2  3
3 
Fig.13.12 1 – osteolytical metastasis MRI; 2 – osteoblastical metastases; 3 – the mixed metastases CT.
Questions for self-control:
1. Classification and roentgenologic diagnostics of the bones tumours|swelling|.
Section 14.
The radio diagnostics of traumatic damages and degenerative-dystrophycal diseases of the musculosceletal system. Drafting of algorithm of radio visualisation of the musculosceletal system.
Section contents:
The radio signs of traumatic damages of bones and joints - fractures, luxationes, types of displacement of fragments, features of fractures of child's and eldery years. The radio signs of normal fracture healing. The complications of fractures healing. The radio signs of degenerative-dystrofical changes of the musculosceletal system, Paget`s disease and uncompleted osteogenesis.
Drafting of algorithm of the musculosceletal system radio visualisation: sciagraphy, radiometry, radionouclide scanning, scintigraphy, computer tomography, magnetic-resonance image, SPECT, PAT, sonography.
The principles of roentgenologic visualisation in traumas of the skeleton:
- on a radiography affected area and the joints near with affected area must be represented;
- the roentgenography (X-ray film) must be made in 2nd mutually perpendicular projections (for example, scigram in frontal and lateral views);
- the first radiography is made together with immobilization material (junk ring, splint) - diagnostic picture (see fig 14.1);
- after reposisition of fragments a control radiograph is made;
- in the unclear case the radiography of symmetric area of the skeleton is made.


Fig.14.1 Diagnostic and control sciagrams of the injured extremity.
The fracture is the violation of integrity of a bone along its entire perimeter.
Fissure is the violation of integrity of a bone is broken not more, than on the half of its perimeter.
Incipient fracture is the violation of integrity of a bone more than on a half, but not on full length of the perimeter.
Classification of fractures
Complete, uncomplete (fissures).
1. According to an operating factor: gunshot fracture, nongunshot, pathological (see fig 14.2);
1  2
2  3
3 
Fig.14.2 1 – not gun-shot fracture; 2 – gun-shot fracture; 3 - pathological fracture
2. By the mechanism of damage: compression (from the compression), torsion (from the wring), flexion (from bending), and avulsion (from spinning out).
3. By the character of line of the fracture: longitudinal, transversal, oblique, spiral, stellate, double, impacted, T-fracture and U-fracture, perforating (see fig 14.3).
Fig.14.3 Direction of fracture lines: a – transversal, b– oblique, c - longitudinal, d – T-fracture, d – Y-fracture
4. By localization: diaphysial, epiphysial, metaphysial, intraarticular.
5. By the plane of the fracture: fragmental, multiple (of one bone).
The roentgenological signs of fracture : fracture line, displacement of fragments, deformation of compact layer, disorganization of trabeces of spongy bone, deformation of the growth plate and dislocating of the ossific nucleus (in children) (see fig 14.4).





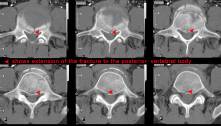
Fig.14.4 Signs of fractures.
Types of displacement of fragments (see fig 14.5).
1. Lateral (on a width) displacement can be complete and uncomplete. In uncomplete displacement one determines what part of diameter of bone fragments were displaced on (on 1/2, on 1/3 and other).
2. Longitudinal displacement - with divergence (diastasis) or with overrriding of bone fragments.
3. Displacement angle-wise. The size of angle of displacement is determined in the point of intersection longitudinal axes of fragments.
4. Displacement on periphery (with rotation) - distal fragment revolves about long bone axis.
Fig.14.5 Types of displacement: a – lateral, b – longitudinal with overriding of bone fragments, c – longitudinal with diastasis of bone fragments, d – impacted fracture, e – angle-wise, f – with rotation.
Date: 2014-12-28; view: 4602
| <== previous page | | | next page ==> |
| The radio diagnostics of inflammatory diseases of the musculoskeletal system | | | Age-related features of fractures |