CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
The purpose of the work
The purpose is to improve methods of management strategies for macrosomia by predicting birth trauma on the basis of comprehensive assessment of external pelvimetry, anthropometry and ultrasonic fetometry.
Materials and methods
254 cases of macrosomic births in Chita Perinatal Center during 2012-2014 were retrospectively analyzed and enrolled in the main group. The control group included 100 pregnant women with suspected fetal weight less than 4,000 g. Subjects of both groups were of the same age and parity births.
Statistical processing of the data obtained was carried out by the software package Statistica 6.0. The data are presented as medians and interquartile scope (25th and 75th percentiles), the average value and confidence interval. Two independent groups were compared by the Mann-whitney U-test, three - with Kraskal-wallis test, followed by Mannwhitney test of paired group comparison and additional Bonferroni adjustment in assessing p value. To assess statistically significant differences in the data we used Student test, with the critical level of significance (p≤ 0.05). The analysis of the differences in the frequencies of two independent groups was performed with the help of Fisher’s exact test with two-sided confidence level, and chi-squared analysis with Yates`s correction. The analysis of prognostic models was conducted using linear step-by-step regression in SPSS Statistics Version 17.0. Then we calculated adjusted determination coefficient to indicate the proportion of explained dispersion. To determine the diagnostic value of the predictive models we used ROC curve with subsequent determination of the area under it [2].
The results
The deliveries were on the 39th – 41st week in 84% of cases (the main group) and in 79% (control group). 55% of the women in the core group gave birth to boys , in the control group the ratio of boys and girls births was 44% and 56%, respectively. The primiparous were 34 %, the secundiparous - 66% of women. The structure of extragenital diseases in the main group revealed the prevalence of alimentary - constitutional obesity (ACO) - 48% and gestational diabetes mellitus (gDM) 10%. In the control group, these indices were 12% and 4%, respectively (p<0.05). Among complications of pregnancy pre-eclampsia was found to account 16% of patients with macrosomia, that index was 1.5 times lower than in the control group (p<0.05). gestational edema in the group with fetal macrosomia twice exceeded those indicators in the control group (p<0.05), which primarily related to disturbance of uteroplacental blood flow. 24% of pregnant women of the main group underwent cesarean delivery. 76% of women were suggested vaginal delivery. In 62% of women with fetal macrosomia delivery was complicated by untimely rupture of amniotic fluid: premature rupture of amniotic fluid (PIV) - 45%, early rupture of amniotic fluid (RIV) - 17%. In the control group untimely rupture of amniotic fluid was registered only in 26%: PIV - 20% (p<0.05), RIV - 6% (p<0.05). Primary delivery weakness in the pregnant with macrosomia was 22%, secondary delivery weakness –16%, discoordinated labor activity - 6%. In the control group the figures were as follows: 8% (p<0.05), 4 % (p<0.05) and 7 % (p>0.05), respectively (Fig.1).

Fig. 1. Frequency anomalies of labor activity in the studied groups
Intrauterine fetal hypoxia was revealed in 38% of cases in the main group, which was twice higher than in the control group 20% (p<0.05). The births of babies with asphyxia of various severity were observed in 24% of women of the main group, and in 12% (p<0.05) in the control one. The frequency of shoulder dystocia in the main group was 6% in symmetric form of macrosomia, and 1% in the asymmetric form. The ratio of the fetus head size to the biacromial diameter mainly contributes to the development of shoulder dystocia (Fig. 2).

Fig. 2. The dependence of shoulder dystocia on ratio of the fetus head size to the biacromial diameter
However, this formula calculates only absolute and relative mathematical values, without taking into account the possibility of displacement of the shoulder axis due to mobility of the sternoclavicular joint. The variability of the displacement of shoulder axis depends on the range of free movements of the fetus chest and the shoulder girdle in the pelvic cavity [3], which directly correlates not only with the cross-sectional area of each pelvic plane, but, with the cross-sectional area of the fetus head segment that passes the birth canal [6] (Fig. 3).

PR - straight size of previus head segment
BPR - the large transverse size of the head
PSRg - anterior-posterior dimension of the fetus chest
PDP - biacromial diameter
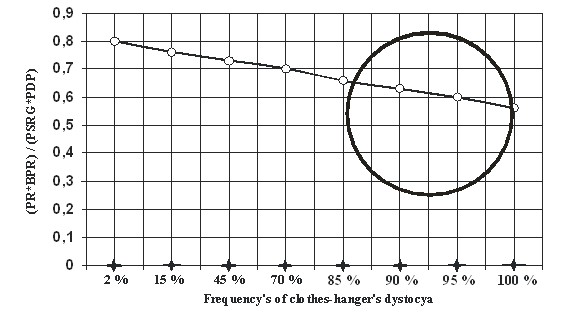
Fig. 3. The dependence of the frequency of dystocia shoulders from the relationship works direct and transverse dimensions of the head of the fetus to the work of the anterior - posterior and transverse dimensions of the shoulders of the fetus
Birth injuries of the fetus in the main group was 47%: injuries of the cervical spine (CS) - 22%, collarbone fracture -16%, cephalohematoma - 8%, intraventricular hemorrhage - 1%. In the control group birth injuries accounted for 11 %: CS injury - 6% (p<0.05), cephalohematoma - 5% (p>0.05). Cerebral ischemia in the neonatal period was diagnosed in 38% of newborns of the main group that is 3 times higher than in the control one (p<0.05) (Fig. 4).
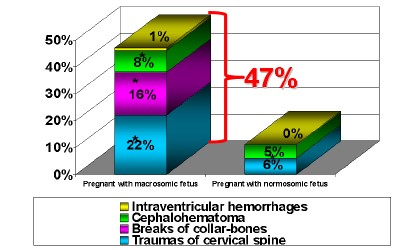
Fig. 4. Frequency of birth injuries in the studied groups
Indications for emergency caesarean section were revealed in14% of the parturient of the main group in the first stage of delivery. Only 34% of vaginal delivery had a favorable outcome for the newborn in the main group. 95% of these women were secundipara, the period of delivery onset did not exceed 39 weeks, in 78% of cases the sex of the fetus was female, the form of macrosomia was symmetric (90%), ACO was not higher the first degree, stable glycemia values were observed during the pregnancy (<5.6 mmol/l) [1].
A Delphi programme was created to analyzes antenatal clinical compliance of the fetus and pelvic planes on the basis of the data of the external pelvimetry, anthropometry and ultrasonic fetometry.
Delphi is an imperative, structured, object-oriented programming language, ObjectPascal dialect. The Delphi Programme consists of program title (program NewApplication), Uses module fields (for example, Useswindows, Messages, SysUtils, and so on), which may not be within the structure and units descriptions and performance ( they begin with compound statement begin and finishes with end). The description blocks are the data of external pelvimetry, anthropometry and ultrasonic fetometry. Blocks of the execution is the conclusion about the clinical compliance of the fetus head to the pelvic planes, and the probability of shoulder dystocia in the fetus. The result is the calculation of the probability of developing birth trauma in macrosomic fetus on the basis of mathematical modeling [5].
The Delphi programme was used in prospective analysis of 54 case reports of deliveries in the City Maternity Hospital during 2013-2014. The prognostic assessment of the development of birth injuries in macrosomic babies determined more frequent indications for caesarean section and resulted in the decrease in CS injuries by 15 % (p<0.05) in the experimental group, fractures of the clavicle by 14 % (p<0.05) (Fig. 5).
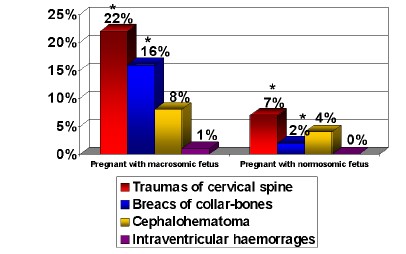
Fig. 5. The efficiency of the method in decrease of birth injuries in the studied groups
Conclusion
Prognostical favorable factors for natural delivery of macrosomic fetus are: delivery in history, the gestation period not more than 39 weeks, the symmetric form of macrosomia, no more than first degree ACO, stable glycemia value during the pregnancy (<5.6 mmol/l) [4].
The ratio of the fetus head size to the biacromial diameter mainly contributes to the development of shoulder dystocia. This ratio may be a criterion for the indication of natural delivery of macrosomic fetus. Thus, the prediction of shoulder dystocia and rational management strategies for macrosomia help to avoids perinatal deaths and significantly reduce birth injuries.
Reference list
1. Krasnopolsky V.I. gestational diabetes a new look at an old problem / V.I. Krasnopolsky,
V. A. Petrukhin, F.F. Burangulova //Obstetrics and gynecology. - 2010. - No. 2. - P.3-6. 2. Levin I.A. Methodology and practice of data analysis in medicine: a monograph. Volume I. Introduction to data analysis / I. Levin, IB Manukhin, YU.N.. Ponomareva V.g., Shemetov - Moscow-tel-Aviv: APLET, 2010. - 168 p.
3. Merz Eberhard. Ultrasound diagnosis in obstetrics and gynecology. In 2 volumes. Volume 1: Obstetrics: Per. s angl. / Eberhard Merz; Ed. by A.I. gus.- M: Medpress-inform, 2011. - 720 p.
4. Patent No. 2496416, Russian Federation, IPC A61 B5/107. The selection method of delivery in pregnant large fetal / M.N. Mochalova, E.V. Kazantseva, E.S. Akhmetova, V.A. Mudrov; applicant and patentee of the State budgetary educational institution of higher professional education Chita state medical Academy No. 2012124614/14; Appl. 14.06.12; publ. 27.10.13, bull. No. 30. - 1 p. 5. Flaman M. The Bible Delphi / M Fleeman - St. Petersburg: BHV-Petersburg, 2011. - 686 p.
6. Chernukha, E.A. Anatomically and clinically narrow pelvis / E.A. Chernukha, A.I. Volobuev, B.E. Puchko - M: Triada-x, 2005. – 186p.
Date: 2016-04-22; view: 1575
| <== previous page | | | next page ==> |
| Choose the best words to complete the sentences. | | | Welcome your audience |