CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
Operation
Embolectomy
As mentioned previously, the most common site for embolic obstruction is the brachial artery.
The arm is placed on an arm table. We prefer to perform embolectomy using local anesthesia. Often a transverse incision placed over the palpable brachial pulse can be used. If proximal extension of the incision is required, this should be done in parallel with and dorsal to the dorsal aspect of the biceps muscle. It has to be kept in mind that 10–20% of patients may have a different brachial artery anatomy. The most common variation is a high bifurcation of the radial and ulnar arteries, and next in frequency is a doubled brachial artery.
An alternative location for embolectomy in the arm is to expose the brachial artery in the bicipital groove. A longitudinal incision starting 10 cm above the elbow that is extended proximally is then used.
If it is hard to achieve a good inflow, a proximal lesion may cause the embolization or thrombosis. More complicated vascular procedures are then required to reestablish flow. The embolectomy attempt is then discontinued and the patient taken to the angiography suite for a complete examination. If practically feasible, an alternative is to obtain the angiogram in the operating room. Frequently, however, the preferred treatment is endovascular, and this is better done in the angiography suite. Occasionally the films will reveal a proximal obstruction that needs open repair. Examples of such are carotid-subclavian, subclavian-axillary, and axillary-brachial bypasses.
Embolectomy via the Brachial Artery
Brachial Artery in the Upper Arm
The incision is made along the posterior border of the biceps muscle; a length of 6–8 cm is usually enough.
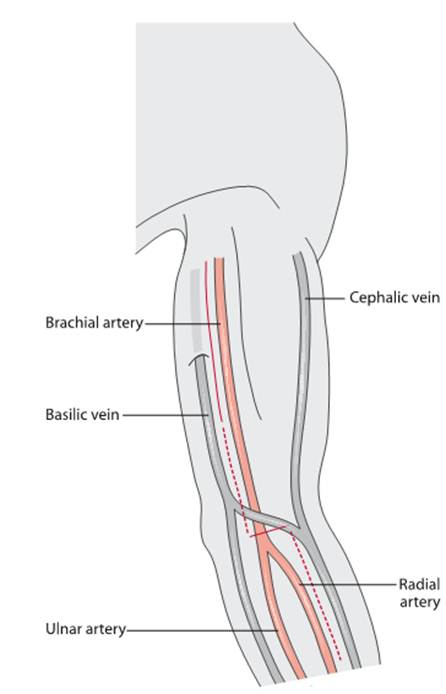
Fig. Transverse incision in the elbow for exposing the brachial artery and with possible elongations (dottedlines) when access to the ulnar and radial branches as well as to more proximal parts of the brachial artery is needed
The muscles are retracted medially and laterally, and the artery lies in the neurovascular bundle immediately below the muscles. The sheath is incised and the artery freed from the median nerve and the medial cutaneous nerve that surrounds it.
Date: 2014-12-29; view: 1196
| <== previous page | | | next page ==> |
| TOPIC 9. ARTERIAL TROMBOSIS AND EMBOLISM | | | ACUTE LEG ISCHEMIA |