CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
Hydrocephaly
Hydrocephaly is a pathological state in which an excessive accumulation of cerebrospinal liquid in the cranial cavity takes place.
A surplus accumulation of CSF is the result of disorder of the functioning of the system of its production and absorption, as well as disorders of its flow within the systems of CSF circulation.
The general volume of CSF in the ventricles and subarachnoid space of the brain varies within the limits of 130-150 ml. Every 24 hours, after different data, from 400 to 800 ml of cerebrospinal liquid is produced. Consequently, it gets renewed several times during 24 hours. The pressure of CSF within the limits of 100-200 mm of water column, measured in the position of patient's lying sideways, is considered normal.
About two-third of the volume of CSF is produced by the vascular plexus of the ventricles of the brain, the rest of it - by ependima and arachnoid membranes. The passive secretion of CSF takes place by the free displacement of ions and other osmotically active substances outside the vascular bloodstream, that conditions the conjugated transition of molecules of water. The active secretion of CSF requires energy consumption and depends on the work of ATP-dependent ionic interchangers.
Absorption of CSF takes place in located parasagitally multiple granulations of the arachnoid membrane - peculiar outpouchings into the cavity of venous collectors (e.g. a sagittal sinus), as well as by vascular elements of arachnoid membranes and arachnoids of the spinal cord, parenchyma and ependima, along the course of connective tissue compartments of cranial and spinal nerves. At that, the absorption is performed both actively and passively.
The speed of producing CSF depends on the perfusion pressure in the brain (the difference between the mean arterial and intracranial pressure), while the speed of absorption is determined by the difference between intracranial and venous pressure.
Such a dissonance generates the instability of the system of CSF dynamics.
The mechanisms providing CSF flow by the system of CSF circulation include the overall of hydrostatical pressures because of the production of CSF, a vertical position of the body, pulsations of the brain, as well as the motion of the villi of ependima.
Within the limits of the ventricular system there are a few narrow areas where the occlusion of the tracts of CSF circulation occurs most often. Here belong a pair Monroe's foramen between the lateral and IIId ventricles, the aqueduct of the cebrum, a pair Lyushka's aperture in the lateral horns of IVth ventricles and an odd Magendie's aperture located in the area of the caudal end of IVth ventricles. Through the three last apertures CSF arrives in the subarachnoid space of the large cistern.
In these areas of the gastric system occlusion of ways of CSF circulation arises most often.
The increase of the amount of CSF in the cerebral cavity can take place because of the disturbance of the balance between its production and resorption, as well as due to the disturbance of its normal outflow.
In 1931, a famous neurosurgeon W. Dandy suggested the classification of hydrocephaly which has been used by the present time and reflects mechanisms of excessive accumulation of CSF. According to this classification, they distinguish the closed (occlusive - arises because of disorder of CSF flow within the ventricular system or on the border between the ventricular system and subarachnoid space) and open (communicable - arises because of the disturbance of the balance between the production and resorption of CSF) of hydrocephaly.
Occlusive hydrocephaly is subdivided into monoventricular (occlusion at the level of one of Monroe's foramina), biventricular (occlusion at the level of both Monroe's foramina, the anterior and middle part of IIId ventricle), triventricular (occlusion at the level of the aqueduct of the brain and IVth ventricles) and tetraventicular (occlusion at the level of Lyushka's and Magendie's apertures). In its turn, the open hydrocephaly can have hypersecretory, hyperresorptive and mixed forms.
Among the reasons causing a persistent occlusion of the tracts of CSF circulation it is necessary to distinguish their innate underdevelopment (the presence of membranes, obturating, Monroe's, Lyushka's or Magendie's apertures, agenesis of the aqueduct of the cerebrum), a cicatrical deformation after the survived CCT or inflammatory process (meningoencephalitis, ventriculitis, meningitis), as well as the compression by a voluminous formation (tumour, aneurysm, cyst, hematoma, granulations, and others).
Hyperproduction of cerebrospinal liquid is an isolated reason of hydrocephaly only in 5% of cases and arises against the background of inflammatory processes in ependima at ventriculitis, against the background of subarachnoid hemorrhage, as well as in the presence of tumour of the ventricular plexus, ependimas. The decrease of the resorption of CSF can take place because of the persistent increase of venous pressure in the upper sagittal sinus as a result of the disorder of the possibility of the system of venous outflow, as well as in a cicatrical deformation of subarachnoid spaces, inferiority of the membrane apparatus or surpressing of the function of its enzymatic systems responsible for the absorption of cerebrospinal liquid.
Thus, after an etiologic sign it is possible to distinguish a hydrocephaly innate, postinflammatory, tumoural arisen on the ground of vascular pathology, as well as of an unknown etiology.
The development of communicable hydrocephaly results in the formation of the so-called internal hydrocranium that is accumulations of CSF mainly in the cavities of the ventricular system at the persistence of its free ambulation along the whole system of CSF circulation. Such a peculiarity of the course of the open hydrocephaly is explained by uneven distribution of tangentially and radially oriented forces in relation to the cerebral cortex in the conditions of an increase of the pressure of CSF. The predomination of the tangentially oriented forces results in the tension of the cerebral cortex and ventriculomegaly.
In accordance with this, they distinguish external and internal forms of hydrocephaly.
Depending on the size of CSF pressure, one distinguishes the hypertensive, normotensive, and hypotensive forms of hydrocephaly. From the point of view of the dynamics of disease progressive, stationary and regressive, as well as active and passive forms.
In clinical relation, important is the distinguishing of compensated and decompensated forms of hydrocephaly. Under decompensated they understand hypertensive hydropsy, occlusive, and progressive hydrocephaly. To the compensated form it is possible to refer stationary or regressive hydrocephaly, as well as normotensive hydrocephaly.
Clinical picture. Hydrocephaly can arise in any age, but most frequently - in the early child's one. If the accumulation of CSF takes place before the coming of the adhesion of cranial bones, there is a gradual, anticipating the age norm increase of the circumference of the head, that results in deformation of the skull. Paralelly, the atrophy or stop in the development of tissue of large hemispheres takes place. For that reason the increase of intracranial pressure either softens or levels fully. In case of a long-term course of such a process, the characteristic picture of normotensive hydrocephaly with large dilated ventricles and apparent atrophy of the cerebral substance is formed.
In some cases one observes the so-called passively developing hydrocephaly at which the pressure of CSF remains initially normal, and a leading link of the process is a progressive atrophy of cerebral tissue because of the survived intracranial hypoxia of the brain, severe craniocerebral trauma, ischemic stroke, endogenous atrophies of the cerebral substance (e.g. in Peak's disease).
In the conditions of hypertensive ventriculomegaly, the tension of conductive ways bending round the ventricles of the brain, their demyelination and by virtue of this the disturbance of possibility which is the reason of the development of motor disorders. At that, frequently revealed in patients paraparesis is explained by damage of the paraventricular part of the pyramidal tract.
The hydrostatical gravity pressure of CSF on the basilar parts of brain, in particular on the hypothalamic area, subcortical nodes, optic nerves and tracts underlay visual disorders, subcortical dysfunction and endocrine disorders.
The chronic increasing of the intracranial pressure, long-term ischemia of brain tissue arising at that, the disturbance of the possibility of associative fibers of large hemispheres against the background of a direct influence of the factor causing hydrocephaly, in sum determines the development of intellectual-mnestic, psychical and endocrine disorders.
The appearance of a child with hydrocephaly is characteristic. The increase of the circumference of the head, its sizes, especially in the sagittal direction, at the persistence of the diminutiveness of the face. The skin on the surface of the head is thinned, atrophic, multiple dilated venous vessels are visible. The cranial bones are thin, the intervals between them are enlarged, especially in the area of the sagittal and coronal sutures, the anterior and posterior fontanels are dilated, tense, sometimes protruding, do not pulsate, a gradual spread of not yet ossified sutures is possible. In percussion of the cerebral part of the head, one can hear the sound of a "cracked pot".
For hydrocephaly of the early child's age, the disorder of the motor innervation of an eyeball is characteristic: a fixed turning of the look downwards (the symptom of the sunset), convergent strabismus against the background of visual acuity up to the formation of a complete blindness. Sometimes motor disorders are accompanied by the development of hyperkinesias. Cerebellar symptomatology becomes apparent a little bit later by the disturbance of statics, coordination of motions, impossibility of keeping the head, sitting, standing. A long-term increase of intracranial pressure, atrophy of cerebral substance can result in a severe deficit of mnestic functions, lagging behind in intellectual development. In the general state of the child, hypererethism, irratibility or, vice versa, adynamy, indifferent attitude toward his/ her people can predominate.
In adults, a leading element of the clinical picture of hydrocephaly is the manifestation of the hypertensive syndrome.
Diagnostics and treatment. Diagnosis of hydrocephaly is now possible to make with a high degree of reliability on the basis of findings of MRI- or CT-investigation. In most cases, the findings of these methods of visualization are quite enough for getting a clear idea of the reasons of the development of hydrocephaly. In children of the first year of life, for diagnostics of hydrocephaly neurosonography is widely used.
In certain cases, the use of etiotropic treatment of hydrocephaly is possible. The impossibility of the elimination of the reason of hydrocephaly or a prognosticated low efficiency of etiotropic treatment determines the necessity of the choice of nosotropic or symptomatic treatment, directed above all things at the removal of intracranial hypertension. Conservative methods of treatment, on the whole, are ineffective and only used at the early stages as courses of dehydratation therapy.The basis for all significant methods of treatment of hydrocephaly is a surgical method.
 The main indication for performing surgical treatment is the progress of hydrocephaly in the absence of inflammation of arachnoid membranes. Variants of surgical operations in different forms of hydrocephaly differ substantially. But at that all of them are based on the formation of the w ay of the permanent averting of CSF into one of the media of the organism, where it is by virtue of one or another reason utilized. Thus, in the case of open hydrocephaly, the permanent taking out of the surplus of CSF out of the cerebral cavity is needed. Taking into account that in this case the communication between the compartments of the system of CSF circulation is not disordered, the application of the lumbar-subarachnoid-peritoneal shunting is possible: the connection through the shunt of the lumbar cistern and peritoneal cavity.
The main indication for performing surgical treatment is the progress of hydrocephaly in the absence of inflammation of arachnoid membranes. Variants of surgical operations in different forms of hydrocephaly differ substantially. But at that all of them are based on the formation of the w ay of the permanent averting of CSF into one of the media of the organism, where it is by virtue of one or another reason utilized. Thus, in the case of open hydrocephaly, the permanent taking out of the surplus of CSF out of the cerebral cavity is needed. Taking into account that in this case the communication between the compartments of the system of CSF circulation is not disordered, the application of the lumbar-subarachnoid-peritoneal shunting is possible: the connection through the shunt of the lumbar cistern and peritoneal cavity.
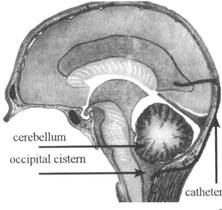
In case of occlusive hydrocephaly, the operation of ventriculocisternostomy has been performed by now (Torkildsen, 1939): mono- or bilateral connection through the shunt of the cavity of the lateral ventricle and the large (occipital) cistern (Fig. 1).
Fig. 1. The scheme of the operation of ventricular shunting in hydrocephaly
Presently, a wide use has been acquired by methods of shunting of the cavity of the lateral ventricle with the canalization of CSF into the cavity of the right atrium (ventriculocardiostomy; Fig. 2) or into the peritoneal cavity (ventriculoperitoneostoiny, used most often; Fig. 3). At that, a shunt is conducted under the skin on a large extent.
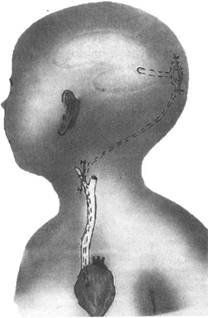
Fig. 2. The scheme of the operation of ventriculocardiostomy in hydrocephaly
It is necessary to note that in case of lumbar-peritoneal, ventriculocardiac and ventriculoperitoneal shunting the construction of the shunt is of particular importance, in which a mandatory element is the valve, unassuming hyperdraining and a reverse flow of liquid, has a special value.
Ventriculostomy (the establishment of a direct communication between the cavity of the lateral or III ventricle and the subarachnoid space) and ventriculocisternostomy results in the compensated course of hydrocephaly in 70% of cases; setting of the shunt system gives an analogical result in 90% of cases.
Complications of the described methods of shunting are the following: occlusion of the shunt at different levels and the formation of its failure(during 5 years after an operation it is revealed in80% of patients); hypo- and hyperdrainage states (in 1/4-1/3 of cases); infecting the shunt (in 4-5% of cases) and the development of ventriculitis, meningitis, meningoencephalitis, and even sepsis; epileptic attacks (in 4-7% of cases); formation of a pseudoperitoneal cyst. All the mentioned variants of complications (except formation of the episyndrome) are the indication for the replacement of the bypass system against the background of performing the proper treatment of the arisen symptomatology.
Recently, in some variants of occlusive hydrocephaly they perform endoscopic operations on the renewal of the possibility of CSF tracts.
Fig. 3. The scheme of the operation of the ventriculoperitoneal by-passing
Date: 2015-02-16; view: 1916
| <== previous page | | | next page ==> |
| Diagnostics of tumours of the spinal cord | | | Types of Task 2 Questions |