CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
Diagnostics of tumours of the spinal cord
 In a number of cases the clinical symptomatology, characteristic of tumours of the spinal cord, can remind the clinical symptomatology at such diseases as osteochondrosis, myelities, arachnoiditis, tuberculosis, spondylitis, discitis, osteomyelitis, syphilis, dissipated sclerosis, ALS, pathology of vessels of the spinal cord and others. Therefore, for performing differential diagnostics and clarification of the nature of the process very important is the use of the data of the anamnesis, dynamics of the development of disease and progress of clinical symptomatology, findings of the objective checkup of the patient, the use of auxiliary methods of investigation.
In a number of cases the clinical symptomatology, characteristic of tumours of the spinal cord, can remind the clinical symptomatology at such diseases as osteochondrosis, myelities, arachnoiditis, tuberculosis, spondylitis, discitis, osteomyelitis, syphilis, dissipated sclerosis, ALS, pathology of vessels of the spinal cord and others. Therefore, for performing differential diagnostics and clarification of the nature of the process very important is the use of the data of the anamnesis, dynamics of the development of disease and progress of clinical symptomatology, findings of the objective checkup of the patient, the use of auxiliary methods of investigation.
Presently, among the auxiliary methods of investigation the most informative are CT and MRI which allow to establish finally the nature of the process and localization of tumour of the spinal cord. In a number of cases, for more exact and reliable information they use MRI with the intravenous contrasting enhancement (Fig. 4).
Fig. 4. MRI at intra- and extramedullar tumours of the spinal cord: a - intramedullar tumour of the cervical part of the spinal cord: b neurinoma of the root of the spinal cord (intra-extravertebral tumour)
They widely use spondylography (roentgenography) of the spine in 2 projections. It is possible to distinguish in spondylograms: calcification, destruction of the vertebra, expansion of intervertebral foramens (at extra-intervertebral tumours; Fig.5), narrowing of the roots of arcs and an increase of the distance between them (Elsberg-Dyke's symptom).
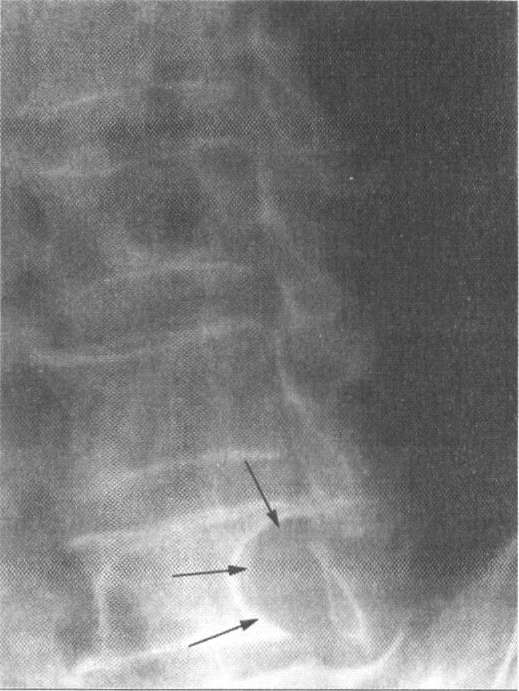
Fig. 55. The roentgenologic picture at the intra-extravertebral tumour (neurinoma) of the spinal cord (the borders of destruction of the bone at the site of the tumor’s growth are pointed out with arrows).
Radionuclide scintigraphy is the method of checkup by rare gases (e.g. Xe), introduced into the organism by a special radiometric apparatus. By the degree of accumulation of radiopharmpreparations in the brain substance, it is possible to judge of the localization and nature of the process, the genesis of disease, especially in cases when performing differential diagnostics is difficult (e.g. in metastases of cancer and inflammatory diseases of the spine - spondylitis, discitis).
The methods of lumbar puncture with performing CSF dynamic tests (Queckenstedt and Stoockey's) for diagnostics of tumours of the spinal cord has been lately used extremely rarely. The revealed CSF dynamic block at Queckenstedt and Stoockey's tests testifies to the compression of the spinal cord and disorder of the possibility of subarachnoid spaces, that in combination with the performed biochemical and microscopic investigations of CSF and discovered protein-cellular dissociation points out a high probability of the presence of tumour of the spinal cord in the patient.
Myelography is roentgenography of the intravertebral content after the contrasting of the subarachnoidale space with a contrast substance (majodilum, lohexol) or gas (oxygen, helium). The method is used for the determination of the level of compression of the spinal cord. By descending myelography it is possible to specify the top level of compression of the spinal cord, and by ascending one - the bottom level. Presently, as a diagnostic method myelography is used rarely in connection with the appearance of more informative, little invasive methods of investigation.
Treatment. The only radical method of treatment of most tumours of the spinal cord is their surgical removal. The earlier is the surgical oncotomy performed, the more favorable will be the postoperative outcome.
The purpose of operation:
1. maximally radical removal of the tumour;
2. maximal persistence of blood supply of tissues of the spinal cord;
3. performing the operative intervention with minimal damage of structures of the spinal cord and its roots, in connection with which surgical approaches depending on localization of tumour (Fig. 6).

Fig. 6. The basic surgical approaches to tumours in different parts of the spine
For the oncotomy of the spinal cord in a number of cases laminectomy is performed according to the level of location of tumour. In, neurinomas the root from which a tumour has grown is coagulated and transected, after which the tumour is removed. Tumours which spread along the root extradurally and outside the vertebral canal are removed with considerable difficulties. Such tumours consist of two parts (intra- and extravertebral) and have a form of "sand-glasses". In such cases for the removal of neurinoma they use combined approaches both from the side of the vertebral canal and from the side of the thoracic or abdominal cavities.
At the removal of meningiomas with the purpose of prophylaxis of relapse of tumour they remove or coagulate the dura mater of the brain from which the tumour was formed. If the tumour is located subdurally, for its removal it is necessary to perform the opening of the dura mater of the brain.
Intramedullar tumours, more frequently, astrocytomas, do not have distinct borders with the spinal cord and considerably spread along, that is why possibilities of their total removal are limited. Removal of intramedullar tumours of the spinal cord must be performed exceptionally with the use of microsurgical technique. After the operation expedient is performing radio- and chemotherapy (the dose of irradiation is selected depending on the histogenesis of the tumour), radiosurgery.
Rehabilitation therapy is performed in the early postoperative period: going in for curative gymnastics, massage of extremities etc. Absolutely impermissible is the use of biostimulators.
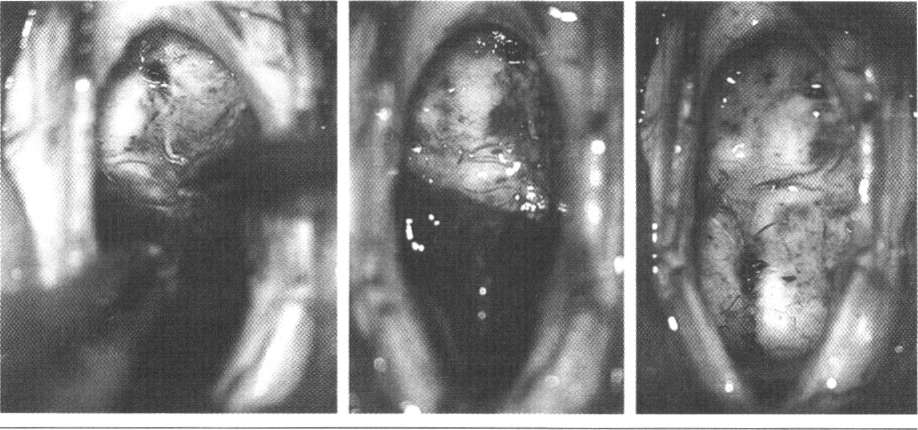
Fig. 7. Stages of the microsurgical removal of tumour of the cervical part
Prognosis. The results of surgical treatment of tumours of the spinal cord depend on the size, histogenesis, localization of tumour, radicalism of the operative intervention. The more apparent are clinical displays and longer the preoperative period, the slower is restoration of disordered functions of the spinal cord in the postoperative period. The earlier and more radical is the operation performed, the better the outcomes of treatment, especially in case of removal of a benign extramedullar tumour of small sizes.
Date: 2015-02-16; view: 2219
| <== previous page | | | next page ==> |
| Tumours of the spinal cord | | | Hydrocephaly |