CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
The main variants of dislocations
Dislocation syndrome of the medial surface of the hemisphere of the brain under the falcate process (semilunar dislocation). At that, part of the callosal gyrus is displaced into a free fissure, formed from below by the corpus callosum, from above - by the free edge of the falcate process. As a result there arises compression of small arterial vessels feeding the indicated area of the brain ipsilateral of the focus of tumour of the anterior cerebral artery, as well as that of the great cerebral vein. The reason of dislocation of such a type is the presence of a voluminous pathological process in the frontal, parietal, rarer - temporal lobe. Most frequently dysfunction of the callosal gyrus does not have apparent clinical manifestations.
Temporotentorial dislocation: dissymetric displacement of mediobasal structures of the temporal lobe (the parahyppocampal gyrus and its hamulus) into Bish's fissure between the edge of the incisure of the tentorium of the cerebellum and the brainstem. It arises as the next stage of the development of the dislocation syndrome in tumours of hemispheric localization. It is accompanied by compression of the oculomotor nerve, displacement downward of the posterior cerebral artery, as well occlusion against the opposite edge of the tentorial opening of the mesencephalon. At that, the ipsilateral pupil first narrows, then gradually broadens to the state of a fixed mydriasis, an eye deviates inwards and ptosis is formed. Later comes a gradual dilatation of the pupil on the opposite side and disorder of consciousness. Disorders of the motor sphere are formed after the type of central hemi-, and further - tetraparesis. There is an alternating Weber's syndrome. Oclusive hydrocephaly is formed. The appearance of decerebration rigidity is possible.
Cerebellotentorial dislocation. It arises not frequently at an apparent increase of pressure in the posterior cranial fossula (in particular, in tumours of the cerebellum) and is characterized by the displacement of tissue of the cerebellum through a fissure in the aperture of the tentorial opening into the middle cranial fossa. Compression effects the superior cerebellar pedincule, superior medullary velum, the plate of the tectum of the mesencephalon, sometimes the brain aqueduct and cisterns of the subarachnoid space of the middle cranial fossa on the side of dislocation. Clinically it becomes apparent by the coming of the comatose state, the paralysis of a look upwards, narrowing of the fixed pupils in safe lateral oculochephalic reflexes, signs of occlusive hydrocephaly.
The dislocation of cerebellar tonsils of the cerebellum into the foramen magnum. More frequently it arises in voluminous processes in the subtentorial space. At that, there is the displacement of cerebellar tonsils in a caudial direction and their dislocation syndrome between the edge of the large cervical opening and medulla oblongata, that inevitably leads to the ischemia of the latter, disorder of breathing, regulation of cardiac activity and as a result - the patient's death.
Diagnostics. The preoperative diagnosis of brain tumour includes the following constituents: nosological diagnosis, topical diagnosis, and pathohistological diagnosis. In suspicion of the presence in the patient of brain tumour, primary is carrying out the general and neurological examination with making the topical diagnosis. It is necessary to consider as concomitant the examination of neuroophthalmologist and otoneurologist, and in suspicion of a metastatic nature of the oncologic process also consultation of other specialists is necessary. A consultation of ophthalmologist is the obligatory condition of the diagnostic process and must include the evaluation of visual acuity, determination of visual fields, investigation of eye grounds. The latter allows to reveal indirect signs of the increase of the intracranial pressure as stagnant disks of optic nerves, their secondary atrophy, and also to define the presence of primary atrophy of optic nerve that can specify the location of the tumour node.
For making a clinical diagnosis obligatory is drawing additional instrumental methods of investigation among which presently the most informing are MRI and CT. (Fig. 2) These methods at modern availability allow to visualize a tumour focus, estimate its sizes and anatomotopographic features, that makes a greater part of the information necessary for the choice of the tactics of surgical treatment. In case of insufficiency of the information got by CT or MRI for the choice of the tactics of treatment, prognostication of its results, as well as for the increase of the quality of surgical intervention, they use methods of angiography (presently considered obligatory in the context of preoperative preparation).
With the purpose of rapid estimation of the degree of the displacement of midline structures, it is possible to use the method of echoencephalography. Such methods as positron-emission tomography (PET), single-photon emission computer tomography (SPECT), electro-encephalography (EEG), Doppler ultrasound are used for specification of the diagnosis.
Roentgenologic methods of investigation (foremost craniography) in diagnostics of brain tumours have presently lost their key significance. The classical roentgenologic signs of the presence of the hypertensive syndrome and brain tumour are osteoporosis of the dorsum sellae and tubercle of the sella turcica, the posterior clinoid process, as well as visualization of an apparent pattern of digital impressions on the internal surface of the bones of the calvarium, diffuse strengthening of canals of diploic veins, distention and deepening of the fossae of pacchionian granulations. In early childhood, the presence of intracranial hypertension results in separation of cranial sutures. The decrease of the bones thickness, as well as the increase of the sizes of its cerebral part.
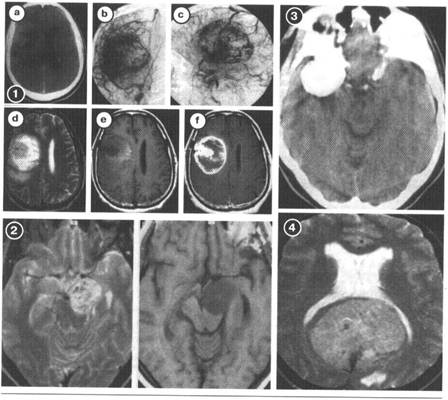 Fig. 2. MRI, CT, AG -picture in different brain tumours: 1 (a-f) glioblastoma of the temporal area of the (MRI is complemented by the findings of angiography); 2 (a-b) neurinoma of VIII pair of cranial nerves; 3 - meningioma of the wing of a sphenoid bone; 4 a giant falx meningioma.
Fig. 2. MRI, CT, AG -picture in different brain tumours: 1 (a-f) glioblastoma of the temporal area of the (MRI is complemented by the findings of angiography); 2 (a-b) neurinoma of VIII pair of cranial nerves; 3 - meningioma of the wing of a sphenoid bone; 4 a giant falx meningioma.
Apart from roentgenological symptomatology of hypertensive osteoporosis of bone tissue, in rare cases one can observe the phenomena of osteolysis or hyperostosis in the areas of growth of certain types of tumours. Sometimes, calcification of areas of tumour or displacement of the calcified pineal body are observed (Fig. 3).
Methods of SPECT and radioisotope scintigraphy allow to define the primary focus at suspicion of the metastatic nature of brain tumour, to estimate some features of biology of tumour and on that basis to specify the supposition about its possible histological type.
The method of stereotaxic needle biopsy of the tumour focus which allows to make an exact histological diagnosis is widely used presently.
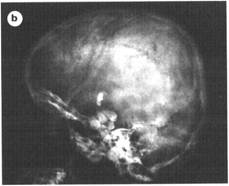
 Fig. 3. Direct roentgenologic signs of brain tumours: a - calcification of olidendroglioma of the parietal area; b - cerebral teratoma (the presence of rudiments of teeth)
Fig. 3. Direct roentgenologic signs of brain tumours: a - calcification of olidendroglioma of the parietal area; b - cerebral teratoma (the presence of rudiments of teeth)
Apart from instrumental methods, it is also possible to use a number of laboratory investigations, such as the determination of hormonal type (at suspicion of the adenoma of hypophysis), a virologic investigation.
 Recently, a liquorological investigation in full (determination of pressure of liquor, its cytological and biochemical composition) is not determining in making the diagnosis of brain tumour, and not infrequently carrying out lumbar puncture is dangerous in view of the danger of the development of dislocation syndrome. Changes of the pressure and composition of cerebrospinal liquid inevitably accompany the development of the tumour process. The pressure of liquor and, consequently, the intracranial pressure can increase 1,2-2 times as compared to normal indicators. As a rule, the degree of the change of intracranial pressure is a little bit lower than the given intervals of extreme upper values. One regards as classical the so-called symptom of protein-cellular dissociation which reflects a considerable increase of the concentration of protein in liquor in the normal or insignificantly increased indicator of the cell number. Such a picture is only observed in case of intraventricular or the dislocation of the tumour node close to the ventricular system. A considerable increase of cells in liquor is observed in malignant neoplasms of the brain with the phenomena of disintegration of tumour nodes (glioblastoma). In this case centrifugation of cerebrospinal liquid allows to get a cellular residue in which in 25% of patients one can reveal tumour cells. In rare cases in the development of hemorrhages into the focus of tumour, in a vast disintegration of the tumour node and the intensive development of the vascular intraventricular tumour liquor may become xanthochromic.
Recently, a liquorological investigation in full (determination of pressure of liquor, its cytological and biochemical composition) is not determining in making the diagnosis of brain tumour, and not infrequently carrying out lumbar puncture is dangerous in view of the danger of the development of dislocation syndrome. Changes of the pressure and composition of cerebrospinal liquid inevitably accompany the development of the tumour process. The pressure of liquor and, consequently, the intracranial pressure can increase 1,2-2 times as compared to normal indicators. As a rule, the degree of the change of intracranial pressure is a little bit lower than the given intervals of extreme upper values. One regards as classical the so-called symptom of protein-cellular dissociation which reflects a considerable increase of the concentration of protein in liquor in the normal or insignificantly increased indicator of the cell number. Such a picture is only observed in case of intraventricular or the dislocation of the tumour node close to the ventricular system. A considerable increase of cells in liquor is observed in malignant neoplasms of the brain with the phenomena of disintegration of tumour nodes (glioblastoma). In this case centrifugation of cerebrospinal liquid allows to get a cellular residue in which in 25% of patients one can reveal tumour cells. In rare cases in the development of hemorrhages into the focus of tumour, in a vast disintegration of the tumour node and the intensive development of the vascular intraventricular tumour liquor may become xanthochromic.
In case of determination of clinical signs indicating an increase of intracranial pressure the dislocation of areas of the brain, and also at the determination of stagnant phenomena on the grounds, carrying out the lumbar puncture is strictly contra-indicated because of a large probability of the dislocation syndrome of cerebellar tonsils into the foramen magnum, that certainly results in the death of the patient.
The features of diagnostics of metastatic tumours is the application of CT and MRI in the mode of contrasting, carrying out stereotaxic biopsy of tumour, performing roentgenography (or CT) of the organs of the thoracic cavity and pelvic cavity, skeletal apparatus, CT of organs of the abdominal region and the pelvic cavity, scintigraphy (of the spine, pelvis and extremities), mammography in women.
Date: 2015-02-16; view: 3511
| <== previous page | | | next page ==> |
| Physiopathology of main symptoms and their clinical display | | | Treatment |