CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
Tumours of hypophysis
Adenomas of the hypophysis are the most widespread tumours of chiasmal-cellular localization and make after different data from 6,7% to 18% of all neoplasms of the brain. The source of tumours of this type are the cells of the prepituitary gland.
After a histological type it is accustomed to distinguish the following variants of adenomas of the hypophysis: acidophilic (somatotropinoma, 13-15%); basophilic (corticotropinoma, 8-10%); prolactinoma (25-28 %); thirotropinoma (1%); gonadotropinoma (7-9%); mixed forms (adenomas which secrete more than one hormone, 3-5%), as well as endocrinologically nonactive adenomas (oncocytoma, adenocarcinoma, nononcocytic adenoma, and others).
After the type of growth they distinguish: infracellar, supracellar, paracellar, antecellar, retrocellar and combined variants of adenomas of the hypophysis.
The main clinical symptoms which arise in adenomas of the hypophysis are:
1. endocrinological disorders conditioned by an increased (rarer - decreased) secretion of hormones;
2. visual disorders conditioned by compression of the chiasma (a decrease of visual acuity, change of visual fields, a more frequent development of bitemporal hemianopsia; the formation of primary atrophy of optic nerves, dysfunction of II, III, IV, VI pairs of cranial nerves);
3. changes of the Turkish saddle (enlargement, its deformation, destruction and others);
4. the formation of the hypertensive syndrome and disturbance of CSF circulation with the development of hydrocephaly.
For the acidophilic adenoma of the hypophysis, an increased secretion of somatotropic hormone is characteristic, that becomes clinically apparent by formation of giantism (in children and teenagers; Fig. 6) or acromegaly (in adults; Fig. 7). For this type of tumour the development of splanchnomegaly (more frequent cardiomegaly; Fig. 8) is characteristic, hyperpiesis (in 25-35% of patients), diabetes mellitus (in 15-19% of patients), dysmenorrhea and amenorrhea in women (70-80% of cases), sexual disorders in men as disturbances of spermatogenesis, atrophy of testicles (30-45% of cases).
For the basophilic adenoma of the hypophysis (corticotropinomas) the increase of secretion of adrenocorticotropic hormone is characteristic. The main clinical displays of hypercorticism are obesity of the upper part of the body, face, presence of pink-purple striae, acne, hirsutism, hyperpiesis, systemic osteoporosis, a disturbance of a menstrual cycle and sexual disorders.
 Prolactinomas are charscterized by the presence of the syndrome of galactorrhea, amenorrhea (in women), sometimes hirsuties, acne (arise because of the activation of the adrenal glands).
Prolactinomas are charscterized by the presence of the syndrome of galactorrhea, amenorrhea (in women), sometimes hirsuties, acne (arise because of the activation of the adrenal glands).

Fig. 6. Giantism in tumours of the hypophysis (a boy at the age of 9 years)
Fig 7. Acromegaly in somatotropinoma of the hypophysis
Diagnostics of adenomas of the hypophysis is also based on the information of a consultation of the endocrinologist and results of the determination of the level of hormones of the hypophysis in blood. Obligatory is a consultation of the ophthalmologist, carrying out MRI or CT of the brain. Aiming craniography of the area of the Turkish saddle has lost its key diagnostic importance.
Fig. 8. Roentgenography of the thorax (cardiomegaly at the somatotropic adenoma of the hypophysis) 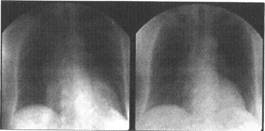 .
.
The treatment of adenomas of the hypophysis includes hormonotherapy, radiotherapy, and surgical methods. The absolute indications for performing surgical intervention concerning the removal of adenoma of the hypophysis are: a progressing decrease of visual acuity of sight, narrowing of visual fields because of the compression of the chiasma and optic nerves, disorder of the motor innervation of the muscular apparatus of the eyesocket, the formation of occlusal hydrocephaly and an increase of intracranial pressure, hemorrhage into tumour, nasal liquorrhea.
The removal of tumours of the chiasmocellar area is performed from the three most often used approaches: transcranial subfrontal (in an apparent paracellar and supraretroantecellar growth), transnasal transphenoidal (used in most cases), and sublabial tanssphenoidal; Fig. 9).
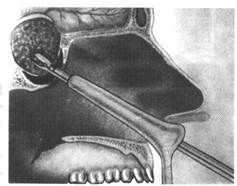
Fig. 9. The transphenoidal approach for the ablation of adenomas of the hypophysis
Radial therapy in treatment of adenomas of the hypophysis is used in a complex with surgical treatment or in the presence of apparent contraindications for carrying out the latter. The most radiosensitive are somatotropinomas. The general dose of a course irradiation makes 45-50Gy.
Date: 2015-02-16; view: 1971
| <== previous page | | | next page ==> |
| Treatment | | | Tumours of the spinal cord |