CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
Treatment
Treatment. At the basis of treatment of brain tumours lies complexity. Presently, in most cases, in treatment of brain tumours surgical, chemotherapeutic and radio-therapeutic methods are used.
Under surgical methods of treatment of brain tumours it is presently necessary to understand carrying out a complete or partial mechanical removal of mass of tumour cells (surgical intervention proper) or initiating acute radiation cytoclasis of tumour cells (radiosurgical interventions).
Chemo- and radiotherapeutic methods of the influence on the tumour focus result in an extended in time death of a certain number of tumour cells, which is of the greatest importance for the decrease of the population of oncogenic progenitors within the normal brain tissue along the periphery or at a distance from the tumour focus.
Surgical treatment of brain tumours includes performing radical operations - directed at a maximally complete oncotomy, as well as palliative interventions carried out with the purpose of diminishing intracranial pressure and extension of the patient's life.
By the degree of completeness a surgical oncotomy can be total, subtotal and partial.
Presently, carrying out surgical interventions on account of oncotomy of the brain requires the use of the newest technological workings out and modern equipment which includes the systems of an optical increase (operation microscopes), systems of intraoperation neurovisualization (MRI and CT plants), systems of the intraoperative roentgenologic monitoring, stereotaxic plants. In a complex, methods of intraoperative visualization allow to carry out the navigation monitoring of the surgeon's actions in relation to the structures of the brain (Fig. 4).
 Fig. 4. Navigational scheme for the implementation of operations on the brain
Fig. 4. Navigational scheme for the implementation of operations on the brain
For the removal of the tumour focus one often uses thermodestruction (laser thermodestruction, cryolysis) and ultrasonic destruction-aspiration.
Radiosurgical destruction of brain tumours is based on performing a single aiming irradiation of the tumour node through the intact skin with the use of radiosurgical plants ƴ-Knife, linear accelerator (Linac), Cyber-Knife and others (Fig. 5). The total dose irradiation of the tumour node makes 15-20g. The spatial error of focusing of ƴ -irradiation for the plant ƴ -Knife does not exceed l,5mm. At that, the sizes of tumour must not exceed 3-3,5 cm in a maximal diameter. Mainly metastatic foci in the brain, meningiomas, and neurinomas are subject to radiosurgical treatment.
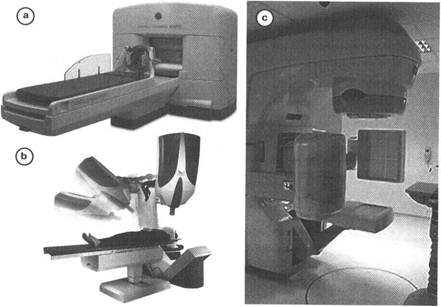
Fig. 5. Types of radiosurgical apparatuses: a - gamma-knife; b - cyber-knife; c -linear accelerator
Palliative treatment of brain tumours (directed at the decrease of the apparency of the hypertensive and dislocation syndromes):
l. surgical methods of decreasing intracranial pressure (among the most effective: external decompression by trepanation of the skull, the internal decompression by the removal of a considerable part of a voluminous tumour focus or resection of brain tissue);
2. renewal of the normal intracranial pressure and the release of the areas of brain tissue involving into the process of dislocation (tentoriotomy in tempotentorial dislocation);
3. renewal of normal CSF flow (CSF-shunting operations: endoscopic ventriculostomy of the 3d ventricle, ventriculocysternostomy, ventriculoperitostomy, ventriculocardiostomy).
Taking into account the main pathophysiological moments of the development of edema-swelling of brain tissue in brain tumours, pathogenetic treatment of these syndromes implies:
1. normalization of the external breathing;
2. optimization of the level of the systemic arterial pressure;
3. facilitation of venous outflow from the cranial cavity (the upper half of the body is raised on the angle of 15° and other conservative ways of a direct or mediated decrease of intracranial pressure (moderate hyperventilation, craniocerebral hypothermia, prescribing osmodiuretics);
Radial therapy is used in subtotal removing of some types of brain tumours or in the complex treatment of malignant tumours. There are different types of this treatment: traditional, hyperfractious, photodynamic therapy, brachitherapy, boron Neutron Capture therapy.
The total dose of irradiation during the course of radiotherapy makes up to 60 gr. The course of radial therapy is appointed in 2 weeks after oncotomy and lasts during 6 weeks with the seances of daily factious irradiation with the dose of 180-200 mgr. The most radiosensitive brain tumours are malignant glioma, oligodendroglioma (in a subtotal resection or in an anaplastic variant), gonadoblastoma, primary lymphadenoma of CNS, medulloblastoma, ependymoma, meningioma (malignant variants, a subtotal or partial removal), adenoma of the hypophysis (after a subtotal removal or in case of ineffectiveness of medicinal therapy), chordoma of the skull base.
Chemotherapy, depending on the method of introduction of the preparation, can be systemic, regional, endarterial (selective), intrathecal and interstitial. The obligatory condition of performing the course of chemotherapy is the preliminary testing of tumour for sensitiveness to the applied preparations. The most chemosensitive are malignant gliomas, primary lymphoadenomas of CNS, tumour infiltrations of arachnoid membrains.
As perspective methods of treatment of brain tumours are presently regarded hormonotherapy (with the purpose of diminishing cerebral edema, and also replacement hormonotherapy), immunotherapy (specific, nonspecific, combined, introduction of monoclonal antibodies, the use of antitumoral vaccines and others), gene therapy.
The treatment of metastatic brain tumours has its own features. In the presence of one metastatic focus located laterally, one performs its surgical removal and appoint the course of radial therapy. At the medial location of a single focus, the application of radiosurgical treatment and appointing a course of radial therapy is indicated.
In the presence of a few foci, among which one focus of large sizes distinguishes itself, which gives a clear clinical symptomatology and is located laterally, one performs its removal and appoints a course of radial therapy. In the presence of three and more foci, application of the radiosurgical method of treatment and appointing a course of radial therapy for the whole area of the head are indicated. In the lateral location of the focus in this case their surgical removal is possible. In the presence of a great number of foci appointing a course of radial therapy is indicated.
Date: 2015-02-16; view: 1766
| <== previous page | | | next page ==> |
| The main variants of dislocations | | | Tumours of hypophysis |