CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
Why does the ulcer appear ? Let remember the physiology of gastric secretion. Physiology of Gastric Secretion
1. U. has experienced a great recession, hyperinflation and drastic falls
2. U. has coal, iron ore, salt, etc.
3. the main branches of U. industry are steel industry, coal and iron mining, chemical industry, electrical industry, machine building etc
4. the volumes of steel produced in our country make it the seventh largest producer in the world.
5. –
6. U. imports chemicals and fuels, machinery and transport vehicles, energy products. It exports tractors, machinery, building materials, consumers goods and crops.
7. domestically produced gas satisfies only 20-25% of total gas demand and oil production meets only10-12% of oil demand.
8. U. plays an important role in the energy security of Europe because 80% of all natural gas goes from Russia and Central Asia to Europe through U. well-developed gas pipeline system.
9. U. should realize its scientific, technological and production potential
10.U. has scientific, technological and production potential
11.U. exports corn, potatoes, sugar etc
12. the livestock cover cattle-breeding, pig-raising, sheep and goats.
13.the agricultural processing sector is regarded as the first priority in the U. economy.
14.new technologies, machinery and skilled specialists affects the level of agricultural productivity.
15.foreign investments in agribussines are rather important for the country`s economy
Why does the ulcer appear ? Let remember the physiology of gastric secretion. Physiology of Gastric Secretion
Hydrochloric acid and pepsinogen are the two principal gastric secretory products capable of inducing mucosal injury. Acid secretion should be viewed as occurring under basal and stimulated conditions. Basal acid production occurs in a circadian pattern, with highest levels occurring during the night and lowest levels during the morning hours. Cholinergic input via the vagus nerve and histaminergic input from local gastric sources are the principal contributors to basal acid secretion. Stimulated gastric acid secretion occurs primarily in three phases based on the site where the signal originates (cephalic, gastric, and intestinal).
- Sight, smell, and taste of food are the components of the cephalic phase, which stimulates gastric secretion via the vagus nerve.
- The gastric phase is activated once food enters the stomach. This component of secretion is driven by nutrients (amino acids and amines) that directly stimulate the G cell to release gastrin, which in turn activates the parietal cell via direct and indirect mechanisms. Distention of the stomach wall also leads to gastrin release and acid production.
- The last phase of gastric acid secretion is initiated as foodenters the intestine and is mediated by luminal distention and nutrient assimilation. A series of pathways that inhibit gastric acid production are also set into motion during these phases. The gastrointestinal hormone somatostatin is released from endocrine cells found in the gastric mucosa (D cells) in response to HCl. Somatostatin can inhibit acid production by both direct (parietal cell) and indirect mechanisms [decreased histamine release from enterochromaffin-like (ECL) cells and gastrin release from G cells. Additional neural (central and peripheral) and hormonal (secretin, cholecystokinin) factors play a role in counterbalancing acid secretion. Under physiologic circumstances, these phases are occurring simultaneously.
The gastric epithelium is under a constant assault by a series of endogenous noxious factors including HCl, pepsinogen/pepsin, and bile salts. In addition, a steady flow of exogenous substances such as medications, alcohol, and bacteria encounter the gastric mucosa. A highly intricate biologic system is in place to provide defense from mucosal injury and to repair any injury that may occur.
The mucosal defense system can be envisioned as a three-level barrier, composed of preepithelial, epithelial, and subepithelial elements. The first line of defense is a mucus-bicarbonate layer, which serves as a physicochemical barrier to multiple molecules including hydrogen ions. Mucus is secreted in a regulated fashion by gastroduodenal surface epithelial cells. It consists primarily of water (95%) and a mixture of lipids and glycoproteins. Mucin is the constituent glycoprotein that, in combination with phospholipids (also secreted by gastric mucous cells), forms a hydrophobic surface with fatty acids that extend into the lumen from the cell membrane. The mucous gel functions as a nonstirred water layer impeding diffusion of ions and molecules such as pepsin. Bicarbonate, secreted by surface epithelial cells of the gastroduodenal mucosa into the mucous gel, forms a pH gradient ranging from 1 to 2 at the gastric luminal surface and reaching 6 to 7 along the epithelial cell surface. Bicarbonate secretion is stimulated by calcium, prostaglandins, cholinergic input, and luminal acidification.
Surface epithelial cells provide the next line of defense through several factors, including mucus production, epithelial cell ionic transporters that maintain intracellular pH and bicarbonate production, and intracellular tight junctions. If the preepithelial barrier were breached, gastric epithelial cells bordering a site of injury can migrate to restore a damaged region (restitution). This process occurs independent of cell division and requires uninterrupted blood flow and an alkaline pH in the surrounding environment. Several growth factors including epidermal growth factor (EGF), transforming growth factor (TGF) α, and basic fibroblast growth factor (FGF) modulate the process of restitution. Larger defects that are not effectively repaired by restitution require cell proliferation. Epithelial cell regeneration is regulated by prostaglandins and growth factors such as EGF and TGF-α. In tandem with epithelial cell renewal, formation of new vessels (angiogenesis) within the injured microvascular bed occurs. Both FGF and vascular endothelial growth factor (VEGF) are important in regulating angiogenesis in the gastric mucosa.
An elaborate microvascular system within the gastric submucosal layer is the key component of the subepithelial defense/repair system. A rich submucosal circulatory bed provides HCO3-, which neutralizes the acid generated by parietal cell secretion of HCl. Moreover, this microcirculatory bed provides an adequate supply of micronutrients and oxygen while removing toxic metabolic by-products.
Prostaglandins play a central role in gastric epithelial defense/repair (Fig. 274-4). The gastric mucosa contains abundant levels of prostaglandins. These metabolites of arachidonic acid regulate the release of mucosal bicarbonate and mucus, inhibit parietal cell secretion, and are important in maintaining mucosal blood flow and epithelial cell restitution.
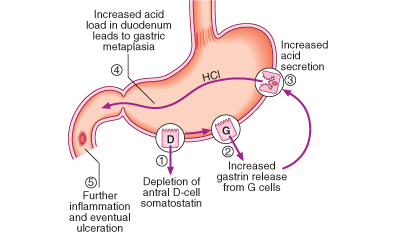
P. Seguence of events in the pathophysiology of duodenal ulceration
PATHOPHYSIOLOGIC BASIS OF PEPTIC ULCER DISEASE
Multiple factors play a role in the pathogenesis of PUD. The two predominant causes are H. pylori infection and NSAID ingestion. PUD not related to H. pylori or NSAIDs may be increasing. Independent of the inciting or injurious agent, peptic ulcers develop as a result of an imbalance between mucosal protection/repair and aggressive factors. Gastric acid plays an essential role in mucosal injury.
PUD encompasses both gastric and duodenal ulcers.
Ulcers are defined as a break in the mucosal surface >5 mm in size, with depth to the submucosa. Duodenal ulcers (DUs) and gastric ulcers (GUs); share many common features in terms of pathogenesis, diagnosis, and treatment, but several factors distinguish them from one another.
Epidemiology
Date: 2014-12-21; view: 6549
| <== previous page | | | next page ==> |
| MARKET CATEGORIES | | | DUODENAL ULCERS |