CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
The levels of closing of deep and surface reflexes
| Reflexes | Muscles | Nerves | Segments |
| Biceps Triceps Carporadial High abdominal Medium abdominal Low abdominal Cremasteric Knee-jerk Achilles Plantar Anal | M.biceps brachii M.triceps brachii Mm. Pronator quadrratus, flexor digitorum, profaudus, brachioradialis, biceps, brachii Mm. Rectus abdominis, transverses abdominis, obliques externus abdominis The same The same M.cremasteric M.quadriceps femoris M.triceps surae Mm.flexor digitorum longus et brevis, flexor hallucis longus M.sphincter ani exterinus | N. musculacutaneous N.radialis Nn.medianus, radialis, musculacutaneous Nn.unersectales The same The same N.genitofemoralis N.femoralis N.ubralis (ischiadicus) N.tibialis Nn.anococcygei | CV-CVI CVII-CVIII CV-CXIII TVI-TVIII TIX-TX TXI-TXII LI-LI LII-LIV SI-SII LV-SI SIV-SV |
Human has a large number of inherent bonds, i.e. unconditioned reflexes fulfilled through the segments of the spinal cord and other parts of the central nervous system. The so-called tonic reflexes are extremely important in the ensuring of the function of the movement. A muscle is tensed even in the outside perception of the impulse of active movement which is indicated by tone. When one stretches the muscle its resistance occurs as a result of coming stress. This phenomenon is called stretch (myotasis) reflex (Gr. myo - muscle, tasis - tension). There is another term - "proprioceptive reflex" (Latin proprius - own) because the irritation of the spiral receptor and the response reflex contraction are within the same muscle.
A new data on electrophysiology of motor function in particular and on the muscle tone have been found in animal experiments. It turned out that the structure of the motor cells of the anterior horns of the spinal cord is not the same thing. The largest of them are designated as small and large α-motor neurons; also there exist γ-motoneurons [R. Granit, 1973].
Large α-motor neurons innervate the white muscle fibres which are capable of rapid contraction (physical). Small α-motor neurons innervate the red muscle fibres which play an important role in maintaining the tone and posture (tonic).
Y-motor neurons are about one third of the anterior horn cells. Axons of α-and γ-motoneurons go to periphery in anterior roots and in peripheral nerves. The axon of α-motorneuron ends with terminate plates on muscle fibres (α-muscular, or extrafusal muscle, fiber). The axon of γ-motor neuron approaches the muscle spindles. So the receptor system is designated, the functional significance of which was found recently. At both ends of the spindle thin muscle fibres (γ-muscle or intrafusal) are put, they end with γ-axons of motor neurons. In the middle (equator) of the spindle a spiral receptor cells of the spinal ganglia is placed. The impulse of γ-motorneuron causes contraction of the muscle spindle elements. It leads to a stretching of its equatorial part and to the irritation of the receptor fibres located here - the endings of the dendrites of cells of spinal ganglia - fibre Ia.
Excitation is transferred to the α-motoneuron, and a tonic muscle tension appears (Pic. 10).
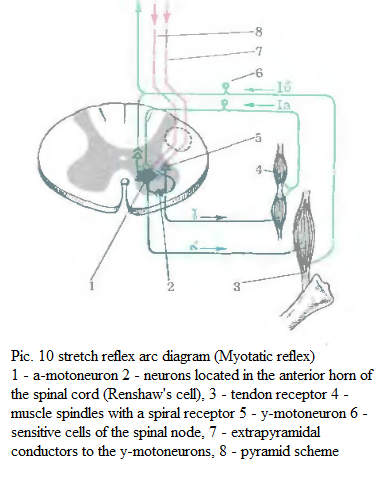 There are central (suprasegmental) links with γ-motoneurons of the spinal cord. They somehow regulate the formation of the stretch reflex. Probably the links begin in the reticular formation of the brain stem, the cerebellum, in the ganglia of the extrapyramidal system. There is a possibility that pyramidal fibres can play this role [R. Granit, 1973]. A part of the dendrites of nerve cells of spinal ganglia of fibres Ib (see Pic. 10) ends up not in the muscle spindle but in the receptors tendons (Golgi tendon organs). They are the receptors for conduction of impulses inhibiting the activity of α-motorneurons. The axons of these sensory neurons end at intercalary cells which are in contact with α-motoneurons.
There are central (suprasegmental) links with γ-motoneurons of the spinal cord. They somehow regulate the formation of the stretch reflex. Probably the links begin in the reticular formation of the brain stem, the cerebellum, in the ganglia of the extrapyramidal system. There is a possibility that pyramidal fibres can play this role [R. Granit, 1973]. A part of the dendrites of nerve cells of spinal ganglia of fibres Ib (see Pic. 10) ends up not in the muscle spindle but in the receptors tendons (Golgi tendon organs). They are the receptors for conduction of impulses inhibiting the activity of α-motorneurons. The axons of these sensory neurons end at intercalary cells which are in contact with α-motoneurons.
The tension generated by the strain muscles causes stimulation of these receptors. They have high limens and are excited only by a significant muscular effort. These action potentials are conducted to the spinal cord and cause inhibition of α-motor neurons. Inhibition of motor neurons of the anterior horn is accompanied by relaxation of synergistic muscles which prevents them from overexertion and by a simultaneous contraction of the muscles-antagonists.
Recent decades neuroscientists and neurohistologists found new data on the structure and function of the so-called proprioneurons (interneurons) of the spinal cord or nerve cells which do not participate in the formation of anterior roots. Renshaw [Renshaw B., 1946] described the special nerve cells called by his name now Renshaw's cells. These cells are located in the anterior horns of the brain and cause inhibitory and sometimes facilitating effect on the α-motoneurons. Before leaving the spinal cord the axon of α-motorneuron gives returning collateral to Renshaw cells. When α-motorneuron has an excess excitation the Renshaw cell has an inhibitory effect (so-called recurrent inhibition). Concerning the role of previously mentioned returning facilitation of α-motorneuron, it alters the interaction between agonist and antagonist muscles; it reduces the effect of the antagonist. Intrafusal muscle fibres can contract under the influence of γ-motoneurons. This increases the excitability of the spiral receptor of the spindle and increases the reflex to stretch the muscles. Under the influence of Renshaw cell the excitability of α-motoneurons changes. That can also reflect the degree of the intensity of stretch reflex. Both of these phenomena can affect muscle tone, which decreases with the affection of the peripheral α-motorneuron. Obviously it depends on the violation of the arc reflex of tension because α-motoneuron is also an effector part of the reflex arc. Muscle tone also decreases when dorsal root is damaged, i.e. when any part of the arc of the segmental reflex is broken.
In clinical practice according to the location of receptors reflexes are divided into the surfacing (skin, from mucous membranes) and into deep (reflexes to muscle strain).
Primarily deep reflex was taken by mistake as a response to direct irritation of the muscle with a reflex hammer on the tendon. Later that point of view of the reflex nature of this phenomenon was adopted. More recently the mechanism of this reflex was represented (also by mistake) in the following way: the reflex hammer irritates the receptor in the tendon which represents the end of the dendrites of nerve cells of spinal ganglia. Arising in this cell the impulse is transferred to the anterior horn of the neuron, the impulse of which reaches the muscles causing contraction and movement. It was established that the tendon reflexes by their nature are identical to the reflections in tension. When one hit with a reflex hammer there is not only the stretch of the tendons, but also the stretch of the muscles. The reflex occurs exactly in response to the stretch. Lengthening of the muscle fiber on a few microns is sufficient to cause it. If stretching is slow, the reflex becomes tonic. A degree of coming at this moment of the muscle tension is the criteria for measuring of its tone. With a short and abrupt irritation by the reflex hammer the reflex becomes "phasic", a reciprocal movement has the character of a single short muscle contraction.
 Currently there is a need to take "tendon" reflexes as one of tension reflexes. The same attributes to so-called peryosteal reflexes. These reflexes are reproduced by the same segmental arch consisting of two neurons - cells of spinal ganglion of α-motorneuron. According to the modern point of view the main agent of "tendon" reflex is the stretch of the muscle spindles. This stretching leads to irritation of the spiral receptor of the cells of spinal ganglia in bursa. Therefore such reflections should not be called as tendon but myotatic or deep. The dual action of α-and γ-neurons in the anterior horns of the spinal cord occurs in the formation of the reflex of the stretch of a muscle. Y-neurons can activate the intrafusal contractile elements under the influence of suprasegmental wires. It eases the formation of a reflex. These deep reflexes are studied on the upper limbs.
Currently there is a need to take "tendon" reflexes as one of tension reflexes. The same attributes to so-called peryosteal reflexes. These reflexes are reproduced by the same segmental arch consisting of two neurons - cells of spinal ganglion of α-motorneuron. According to the modern point of view the main agent of "tendon" reflex is the stretch of the muscle spindles. This stretching leads to irritation of the spiral receptor of the cells of spinal ganglia in bursa. Therefore such reflections should not be called as tendon but myotatic or deep. The dual action of α-and γ-neurons in the anterior horns of the spinal cord occurs in the formation of the reflex of the stretch of a muscle. Y-neurons can activate the intrafusal contractile elements under the influence of suprasegmental wires. It eases the formation of a reflex. These deep reflexes are studied on the upper limbs.
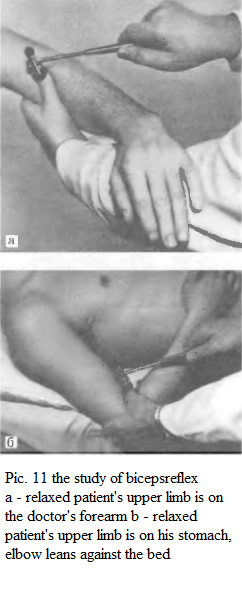
 Biceps reflex is caused by a blow of a reflex hammer on the tendon of this muscle above the elbow. The patient's upper limb bents slightly in this joint (Pic. 11). The muscle contraction and slight flexion of the upper limb at the elbow occur in response to a strike. This reflex is called biceps reflex. Its arc is closed at spinal segments Cv - CVI, afferent and efferent fibers of the reflex arc are in the musculocutaneous nerve.
Biceps reflex is caused by a blow of a reflex hammer on the tendon of this muscle above the elbow. The patient's upper limb bents slightly in this joint (Pic. 11). The muscle contraction and slight flexion of the upper limb at the elbow occur in response to a strike. This reflex is called biceps reflex. Its arc is closed at spinal segments Cv - CVI, afferent and efferent fibers of the reflex arc are in the musculocutaneous nerve.
 Triceps reflex is caused by a blow of a reflex hammer on the tendon of this muscle by 1-1.5 cm above the olecarnon; there are muscle contractions and extension of the upper limb at the elbow (triceps reflex). Ways of induction: 1) the upper limb of a patient is supported at the elbow by the doctor's hand, arm hanging down freely (Pic. 12, a), the doctor supports the bent arm of the patient at the elbow part (Pic. 12b). The reflex arc, the sensory and motor fibers of the radial nerve are closed at SVII - SVIII.
Triceps reflex is caused by a blow of a reflex hammer on the tendon of this muscle by 1-1.5 cm above the olecarnon; there are muscle contractions and extension of the upper limb at the elbow (triceps reflex). Ways of induction: 1) the upper limb of a patient is supported at the elbow by the doctor's hand, arm hanging down freely (Pic. 12, a), the doctor supports the bent arm of the patient at the elbow part (Pic. 12b). The reflex arc, the sensory and motor fibers of the radial nerve are closed at SVII - SVIII.
The wrist–radial reflex is also attributed to deep reflexes of the upper limbs. When one hit with a reflex hammer on the awl-shaped appendix of the radius bone there an elbow flexion and pronation of the forearm occur. Starting position: an upper limb is flexed at the elbow at an angle of about 100°, hand is supported by the doctor in the middle position between pronation and supination (Pic. 13a). This reflex can be investigated with the patient supine (Pic. 13b). Reflex arc is closed at CV - CVIII, the fibre is a part of the median, radial and 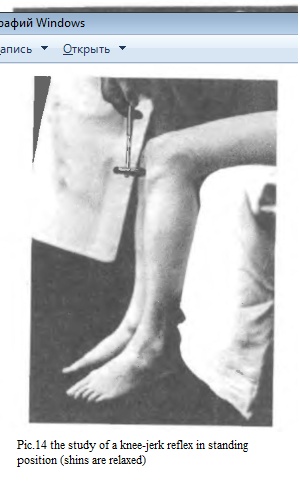 musculocutaneous nerves. The wrist-radial reflex is one of the periosteal reflexes. It is supposed that it is caused by irritation of receptors in the periosteum, but most likely this reflex is attribiuted to myotatic and it occurs because of the stretch of humeroradial muscle, round pronator muscle and biceps.
musculocutaneous nerves. The wrist-radial reflex is one of the periosteal reflexes. It is supposed that it is caused by irritation of receptors in the periosteum, but most likely this reflex is attribiuted to myotatic and it occurs because of the stretch of humeroradial muscle, round pronator muscle and biceps.
Deep abdominal reflexes are caused when one blow with a reflex hammer on the pubic region of 1-1.5 sm to the right and to the left of the centre line in response to contracting muscles of the appropriate side of the abdominal wall. The reflex arc is closed in segments TVII-TXII.
Knee-jerk reaction is an extension of the lower limb at the knee when one strikes the quadriceps tendon below the kneecap. There are several ways to study the knee reflex.
 In the sitting position the patient should put the lower limb to the other or to sit down so that his legs are hanging freely and the angle of flexion of the lower limbs in the knee joints is about 90° (Pic. 14). The patient also can sit in this position: his feet are loosely based on the floor and the lower limbs are bent at the knees at an obtuse angle (Pic. 15). When a patient is lying on his back a doctor brings his left hand under the knee of the patient and places them so that the angle of flexion of the knee joints is obtuse and the heels are freely lean against the bed.
In the sitting position the patient should put the lower limb to the other or to sit down so that his legs are hanging freely and the angle of flexion of the lower limbs in the knee joints is about 90° (Pic. 14). The patient also can sit in this position: his feet are loosely based on the floor and the lower limbs are bent at the knees at an obtuse angle (Pic. 15). When a patient is lying on his back a doctor brings his left hand under the knee of the patient and places them so that the angle of flexion of the knee joints is obtuse and the heels are freely lean against the bed.
Knee reflexes of some healthy people are inhibited and are hardly caused. In such cases they use the Endrashik's method: the patient is offered to couple his fingers of both hands and to pull the hands in both ways with power (Pic. 16). The Endrashik's effect explains the activating effect of γ-neurons on the intrafusal muscle fibres.
The patient's attention is distracted to facilitate the knee-jerk reaction of causing: he is asked questions, he is proposed to count in his mind, to take deep breaths, etc.
The arc of the knee reflex: sensory and motor fibres of the femoral nerve, spinal cord segments LII-LVI.
Achilles jerk is a reduction of the gastrocnemius and plantar flexion of the foot in response to a blow of a reflex hammer on the Achilles tendon. During the examination of the patient when he lies on his back the doctor holds the patient's foot with left hand, bend the lower limb at the knee and hip joints, makes dorsiflexion of the foot (Pic. 17a). When the patient is lying on his stomach his lower limbs are bent at right angle in the knee and ankle joints, and the doctor holds the foot with one hand, with another he blow the Achilles tendon (Pic. 17b). The patient is kneeling on a chair or couch so that his feet are freely hanging, and in this position the doctor makes a blow with a reflex hammer on the Achilles tendon (Pic. 18). Reflex arc: sensory and motor fibers of the tibial nerve, spinal cord segments SI-SII.

Except deep reflexes patients are examined on surface (skin) reflexes.
Abdominal reflexes: the top reflex is caused by the stroke irritation of the stomach skin on parallel rib arch (Pic. 19, 1), medium reflex is caused by the irritation in the horizontal direction at the level of the navel (Pic. 19, 2), the lower reflex is caused along the inguinal fold (Pic. 19, 3 ). Stomach muscles on the 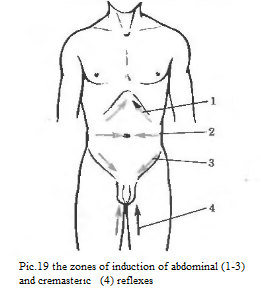 corresponding side contract. The patient lies on his back with a free extended lower limbs. When the patient is a multiparous women with a loose skin in the abdominal area, an obese person or an individual at older age it is recommended to pull the skin of the stomach during examination. Reflex arc passes through the following spinal segments: upper abdominal reflex - TVI-TVIII, average - TIX-TX, lower - TXI-TXII.
corresponding side contract. The patient lies on his back with a free extended lower limbs. When the patient is a multiparous women with a loose skin in the abdominal area, an obese person or an individual at older age it is recommended to pull the skin of the stomach during examination. Reflex arc passes through the following spinal segments: upper abdominal reflex - TVI-TVIII, average - TIX-TX, lower - TXI-TXII.
 Cremasteric (testicular) reflex – the contraction of the muscle that raises the testicle, a stroke irritation of the skin of the inside of the thigh (Pic. 19, 4). Reflex arc is closed in segments LI-LII; sensory and motor fibres are the parts of the genitofemoral nerve. A boy require this reflex at 4-5 months.
Cremasteric (testicular) reflex – the contraction of the muscle that raises the testicle, a stroke irritation of the skin of the inside of the thigh (Pic. 19, 4). Reflex arc is closed in segments LI-LII; sensory and motor fibres are the parts of the genitofemoral nerve. A boy require this reflex at 4-5 months.
Plantar reflex – a plantar flexion of the toes in response to a stroke irritation of the outer edge of the foot (Pic. 20). Spinal reflex arc is closed in segments LV-SII and passes as a part of the sciatic nerve. This reflex begins to be caused only at children older than 2 years, it appears at the possibility to maintain posture when standing or walking.
Anal reflex – the contraction of the orbicular muscle of anus (external sphincter) because of injections around the anus. Scheme of the anal reflex arc - SIV-SV n. anococcygei n. pudendus.
In addition to assessment of the skin surface reflections it is quite informative to study reflexes of the mucous membranes (corneal, palatine and pharyngeal). Methods of their causing are in Chapter 7 (V, IX and X pairs).
When reflexes are being evoked it is necessary to assure the patient to have a complete relaxation to study a limb. Reflex hammer blows should be applied with equal force. Assessing reflexes it's important to pay attention to their intensity and symmetry. Therefore it's necessary to examine the same reflexes from the right and the left sides and to compare them immediately. Intensity of reflexes of healthy people may individually vary, particularly the symmetrical position or recovery of reflexes with fully intact muscle strength can be regarded as a norm.
There are the following changes of reflexes: decrease or loss (if damaged reflex arc), increase and distortion (with the defeat of the pyramidal system and an uninhibition of segmental apparatus of the spinal cord).
CHAPTER 3
Date: 2015-12-11; view: 4178
| <== previous page | | | next page ==> |
| REFLEXES AND THEIR CHANGES | | | THE OVERALL SENSITIVITY AND ITS DISORDERS |