CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
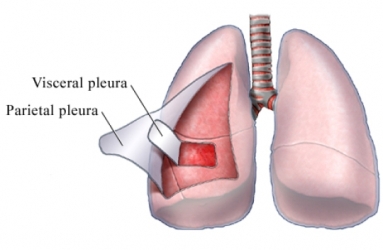
Pleural rub
This is caused by the inflamed surfaces of the pleura rubbing together. The sound has been likened to new leather when it is bent or more vividly to the creaking noises made in a sailing ship heeling to the wind which you may have experienced from films if not in reality. Some idea of the quality of the sound can be obtained by placing one hand over the ear and rubbing the back of that hand with the fingers of the other. Pleural rubs are usually heard on both inspiration and expiration.
At first you may think that you are moving the stethoscope on the chest. Sometimes coarse crackles can sound like rubs; a cough will shift the former. If there is any pain, ask the patient to point to the site of the pain, this often localises the rib too. Rubs are heard in all varieties of pleural inflammation such as in pneumonia and pulmonary embolism. Any effusion will separate the pleura and the rub may well go but sometimes remain above the effusion.
Absent or diminished breath sounds are always an abnormal finding warranting investigation. Fluid, air, or solid masses in the pleural space all interfere with the conduction of breath sounds (pneumonia, pneumo-, hydro-, haemothorax, tumor of lung or mediastinal, emphysema of lungs, atelectasis, airways obstruction, a foreign body in the bronchus). Diminished breath sounds in certain segments of the lung can alert the doctor to pulmonary areas that may benefit from postural drainage and percussion. Increased breath sounds following pulmonary therapy indicate improved passage of air through the respiratory tract.
Voice sounds are also part of auscultation of the lungs. Normally voice sounds or vocal resonance is heard, but the syllables are indistinct. They are elicited in the same manner as vocal fremitus, except that the doctor listens with the stethoscope. Consolidation of the lung tissue produces three types of abnormal voice sounds.
1. Whispered pectoriloquy, in which the child whispers words and the nurse, hears the syllables.
2. Bronchophony, in which the child speaks words that are not distinguishable but the vocal resonance is increased in intensity and clarity.
3. Egophony, in which the child says "ee," which is heard as the nasal sound "ay" through the stethoscope.
Decreased or absent vocal resonance is caused by the same conditions that affect vocal fremitus.
Various pulmonary abnormalities produce adventitious sounds that are not normally heard over the chest. They are not alterations of normal breath sounds but rather sounds that occur in addition to normal or abnormal breath sounds. They are often referred to as the three "R’s": rales (from the French word meaning "rattle"), rhonchi, and rubs. Considerable practice with an experienced tutor is necessary to differentiate the various types of adventitious sounds. Often it is best to describe the type of sound heard in the lungs rather than to try and label it correctly.
Rales result from the passage of air through fluid or moisture. They are more pronounced when the child takes a deep breath. Even though the sound may seem continuous, it is actually composed of several discrete sounds, each originating from the rupture of a small bubble. The type of rales is determined by the size of the passageway and the type of exudate the air passes through. They are roughly divided into three categories: fine, medium, and coarse.
Fine rales (sometimes called crepitant rales) can be simulated by rubbing a few strands of hair between the thumb and index finger close to the ear or by slowly separating the thumb and index finger after they have been moistened with saliva. The result is a series of fine crackling sounds. Fine rales are most prominent at the end of inspiration and are not cleared by coughing. They occur in the smallest passageways, the alveoli and bronchioles.
Medium rales are not as delicate as fine rales and can be simulated by listening to the "fizz" from recently opened carbonated drinks or by rolling a dry cigar between the fingers. They are prominent earlier during inspiration and occur in the larger passages of the bronchioles and small bronchi.
Coarse rales are relatively loud, coarse, bubbling, gurgling sounds that occur in the large airways of the trachea, bronchi, and smaller bronchi. Often they clear partially during coughing. They are frequently heard in dying patients because the cough reflex is depressed, allowing thick secretions to accumulate in the trachea and major bronchi. Because they are so common when death is imminent, coarse rales are often called "the death rattle."
Rhonchi (rales) are sounds produced as air passes through narrowed passageways, regardless of the cause, such as exudate, inflammation, spasm, or tumor. Rhonchi are continuous, since sound is produced as long as air is being forced past an obstruction. Although they are often more prominent during expiration, they are usually present during both phases of respiration. Rhonchi are classified according to pitch as sibilant or sonorous.
Sibilant rhonchi are high pitched, musical, wheezing, or squeaking in character. The wheezing quality is often more pronounced on forced expiration. Sibilant rhonchi are produced in the smaller bronchi and bronchioles.
Sonorous rhonchi are low pitched and often snoring or moaning in character. They are produced in the large passages of the trachea and bronchi. Like coarse rales, they can be partly cleared by coughing. Some clinicians classify sonorous rhonchi as coarse rales, or vice versa.
The other adventitious sound of importance is the pleural friction rub. Its sound can be simulated by cupping one hand to the ear and rubbing a finger of the other hand across the cupped hand. The most common site for a friction rub to be heard is the lower antero-lateral chest wall (between the midaxillary and midclavicular lines), the area of greatest thoracic mobility.
Date: 2015-02-03; view: 1883
| <== previous page | | | next page ==> |
| Vocal resonance | | | Classifacation and mechanism of origin of dry rales |