CATEGORIES:
BiologyChemistryConstructionCultureEcologyEconomyElectronicsFinanceGeographyHistoryInformaticsLawMathematicsMechanicsMedicineOtherPedagogyPhilosophyPhysicsPolicyPsychologySociologySportTourism
Evaluation of Severity of Ischemia
Classiication
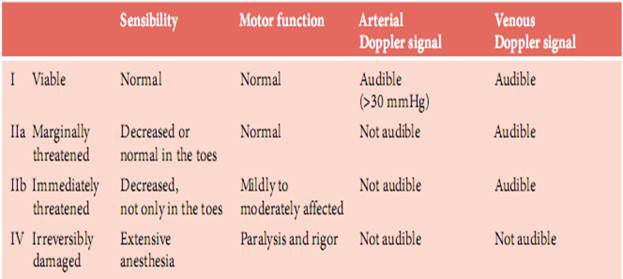
When a patient has been diagnosed to have acute leg ischemia, it is extremely important to evaluate its grade. Ischemic severity is the most important factor for selecting a management strategy, and it also affects treatment outcome. Classification according to severity must be done before the patient is moved to the floor or sent to the radiology department. We have found that the simple classification suggested by the Society for Vascular Surgery ad hoc committee (1997) is helpful for grading. It is displayed in Table 4.
Table 4. Categories of acute ischemia
Viable Leg
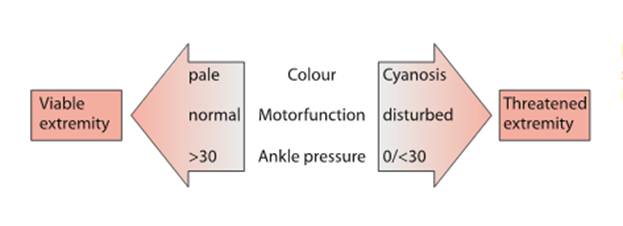
As indicated in Figure 2, a viable ischemic leg is not cyanotic, the toes can be moved voluntarily, and the ankle pressure is measurable. The rationale for choosing these parameters is that cyanosis and impaired motor function are of high prognostic value for outcome. The limit of 30mmHg for the ankle pressure is not important per se but is a practical limit useful to make sure that it is the arterial, and not a venous, pressure that has been measured. The dorsalis pedis, posterior tibial arteries, or branches from the peroneal artery can be insonated. The latter can be found just ventral to the lateral malleolus. If no audible signal is identified in any of these arteries or if there only is a weak signal that disappears immediately when the tourniquet is inflated, the ankle blood pressure should be recorded as zero. It is important to rely on the obtained results and not assume that there is a signal somewhere that is missed due to inexperience. Qualitative analysis of the Doppler signal is seldom useful when evaluating acute leg ischemia.
Fig. 2. Simpliied algorithm to support the management of acute leg ischemia
Threatened Leg
As shown in Table 4, the threatened leg differs from the viable one in that the sensibility is impaired and there is no measurable ankle blood pressure. The threatened limb is further separated into marginally threatened and immediately threatened by the presence or absence of normal motor function. The threatened leg differs from the irreversibly damaged leg by the quality of the venous Doppler signal. In the irreversibly damaged leg, venous blood flow is stagnant and inaudible.
Management Strategy
A viable leg does not require immediate action and can be observed in the ward. A threatened leg needs urgent operation or thrombolysis. The latter is more time-consuming and recommended for the marginally threatened leg. The immediately threatened leg must be treated as soon as possible, usually with embolectomy or a vascular reconstruction. Irreversible ischemia is quite unusual but implies that the patient’s leg cannot be saved. Figure 2 is intended to show a simplified algorithm to further support the management of acute leg ischemia.
Date: 2014-12-29; view: 814
|